Diagnosis?
pseudo aneurysm
pepsi-cola sign that is suggestive of pseudoaneurysm
Cardiologist notes a femoral bruit a few days after performing transfemoral LHC. He calls you asking how likely you are to accurately diagnose a pseudoaneurysm (PSA) w/ DUS imaging.
What to tell him?
DUS is a both sensitive and specific for PSA diagnosis
- 94% sensitivity
- 97% specificity
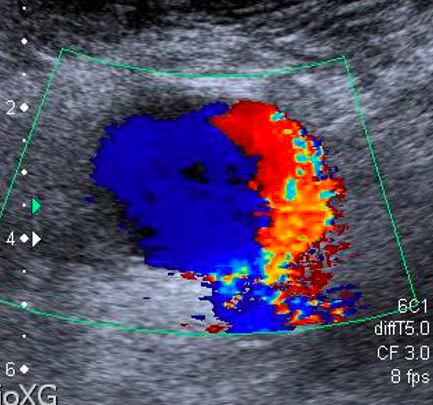
Patient undergoes LE arterial DUS. You come across an isolated image from region near femoral artery (shown below) while reading the study. No further images of the finding are available.
What to do next?
Have tech go back and interrogate region w/ pw
Swirling pattern w/ sack off of common femoral artery should make you think of PSA* (but it is not diagnostic)
pw doppler imaging showing bidirectional flow in sack attached to CFA is pathognomonic of PSA
*PSA = pseudoaneurysm
Low-resistance doppler signal in EIA 3 wks after LHC.
*EIA = external iliac artery
think of AV fistula
low-resistance doppler signal (LRDS) in the proximal iliofemoral arterial system after LHC→ think of AVF
shown below: LRDS in CFA
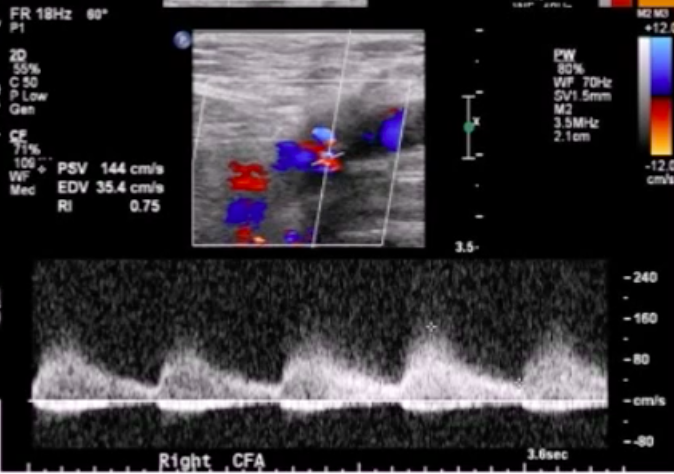
Name five vascular DUS findings that are characteristic of AV fistula.
- markedly increased arterial PSV
- venous pulsatile flow distal to AVF
- arterial LRDS* proximal to AVF
- color bruit
- +/- visualization of fistula tract
*LRDS = low-resistive doppler signal
Patient with vascular Ehlers-Danlos syndrome undergoes arterial duplex study. Pertinent findings shown below. Diagnosis?
Dissection
Frank’s spaghetti is a 60-year-old obese Italian man who comes to your vascular lab for a study prior to initiation of hemodialysis. The ordering physician did not specify what he wants done. What is the most likely reason for patient’s visit to your lab?
Patient likely needs superficial venous ultrasound study [vein mapping] Above is performed in order to see if patient is a candidate for 80 fistula surgery, which is preferred over grafting for HT access
You are performing a vein map study for a patient with new HD. Your tech wants to know how to do the study. What to tell her?
Evaluate the upper extremity veins of the non-dominant arm in the following way: Look at the cephalic vein up to the subclavian vein for compressibility diameter and continuity. May Pl., Turnock it on arm to help bring out Venus structures
Patient who is scheduled for vein mapping has small it’s Reddick cephalic vein. What to do next?
Evaluate basilic system
What is the purpose of evaluating the subclavian an axillary vein’s when doing a vein mapping study?
Want to rule out central venous obstruction.
What size superficial veins in the upper extremity correlate with higher likelihood of fistula maturation with regard to a vein mapping study?
Diameter greater than 2.5 mm
Explain to your tech how to perform the arterial portion of a preop 80 fistula exam
Evaluate brachial radial and ulnar arteries for of the following: Calcification Waveform characteristics (One triphasic flow) Patency (want lumen diameter greater than 2.0 mm) Anatomic variance [high radial artery take off]
Patient with end-stage renal disease on HD has high resistance waveform and left distal subclavian artery. The right subclavian artery has normal flow. Diagnosis?
Probably Access site occlusion or stenosis.
Important components of post AV access creation vascular ultrasound study?
Evaluate inflow artery for stenosis/occlusion Evaluate arterial anastomosis site and beam out and color to look for “swing site” stenosis Evaluate body of access as well as outflow vain for Neil intimal hyperplasia Newly created if you fish Ila should be evaluated for vessel diameter and depth to ensure adequate cannulation
How long to 80 fish is usually take to mature?
3 to 4 months Balloon assisted maturation is an option to speed along the process.
How long before an AV graft can be used after it is placed
Usually 2 to 4 weeks
What is the preferred flow volume rate for an AV graft compared to a navy fistula?
AV graft: greater than 800 mL per minute If you fistula: greater than 600 mL per minute
Role of sixes for AV fistula?
Fistula diameter greater than or equal to 6.0 mm Fistula depth from skin less than 6.0 mm Low-volume greater than 600 mL per minute
Best area to measure flow volume when assessing if you fistula?
Brachial artery It is not ideal to measure outflow vessel diameter to use for calculation for volume; because this can give rise to many Errors
Major pitfall of assessing AV fistula Doppler flow dynamics?
Setting the flow sample size too small and sampling near the wall of the vessel This will lead to underestimation of flow velocity
Formula for estimation of AV fistula flow?
AVF flow equals brachial artery flow -75 200 mL per minute
Patient with 80 fistula has estimated AV fistula flow of 400 mL per minute what to do next?
Recommend that they should have assessment for new AV fistula repair of current fistula Can you foundation recommends replacing 80 fistula Winflo is less than 500 mL per minute
At what value of AV graft flow does the kidney foundation recommend replacing a graft?
600 mL per minute or less
Criteria for AV access site stenosis? Venus anastomosis site.
Greater than 2 to 1 Peak systolic velocity ratio and Greater than 50% lumen reduction. Above refers to proximal site comparison to distal site






