what groups have the highest incidence of diabetes
american indians and alaskan natives followed by hispanic
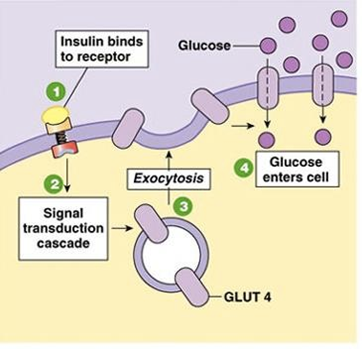
describe insulin
- created in the BETA ISLET CELLS OF THE PANCREAS
- Glucose levels > 70mg/dl cause INCREASE in SYNTHESIS and SECRETION OF INSULIN from the pancreas
- Insulin Binds to cell receptors (TK) leading to a cascade of reactions –> translocation of GLUT4 to cell membrane
–> RESULT in INFLUX OF GLUCOSE, PROTEIN and GLYCOGEN synthesis, cell growth
Type I diabetes
- caused by complete or near complete insulin deficiency (usually seen with >70% destruction of beta cells
- Typically AUTOIMMUNE DESTRUCTION OF BETA CELLS, tend to be young
- genetic, environmental and immunologic factors
- Increased risk of celiac disease, thyroid disease
Type II diabetes
- Results from INSULIN RESISTANCE, abnormal insulin secretion and abnormal fat metabolism
- OBESITY, family history, sedentary lifestyle, HTN, dyslipidemia, etc is a risk factor
- STRONGER GENETIC COMPONENT
- Preceded by progressive insulin resistance
–> impaired fasting glucose, imapired glucose tolerance
–> metabolic syndrome (HTN, HLD, obesity)
Symptoms of diabetes
- Frequent urination
- always tired
- always hungry
- sexual problems
- weight loss
- wounds that won’t heal
- vaginal infections
- numb or tingling hands or feet
- always thirsty
- blurry vision
** THE ONSET OF SYMPTOMS can be SLOW and INSIDIOUS, esp in pts with type II DM**
When should you screen
- screening individuals every 3 years starting at 45 years of age
- Sceen earlier if patients is overweight with at least one additional risk factor (HTN, PCOS, SEDENTARY etc)
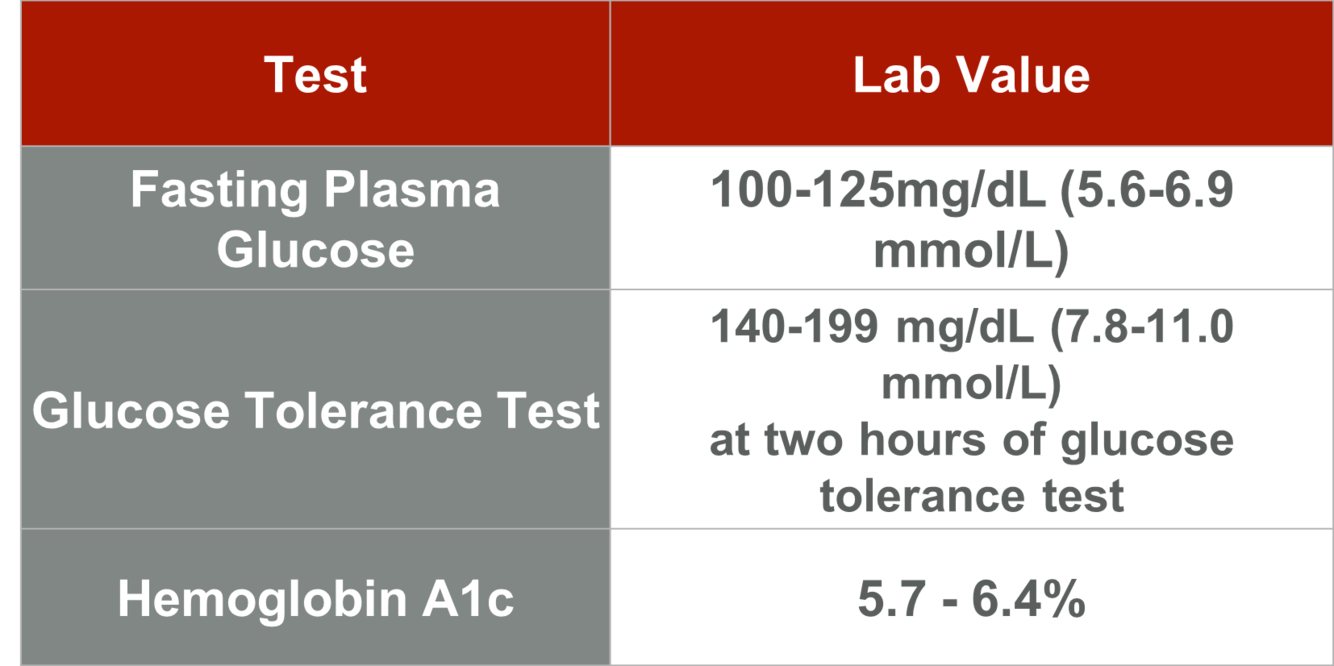
Prediabetes
- increased risk of diabetes or intermediate hyperglycemia
-
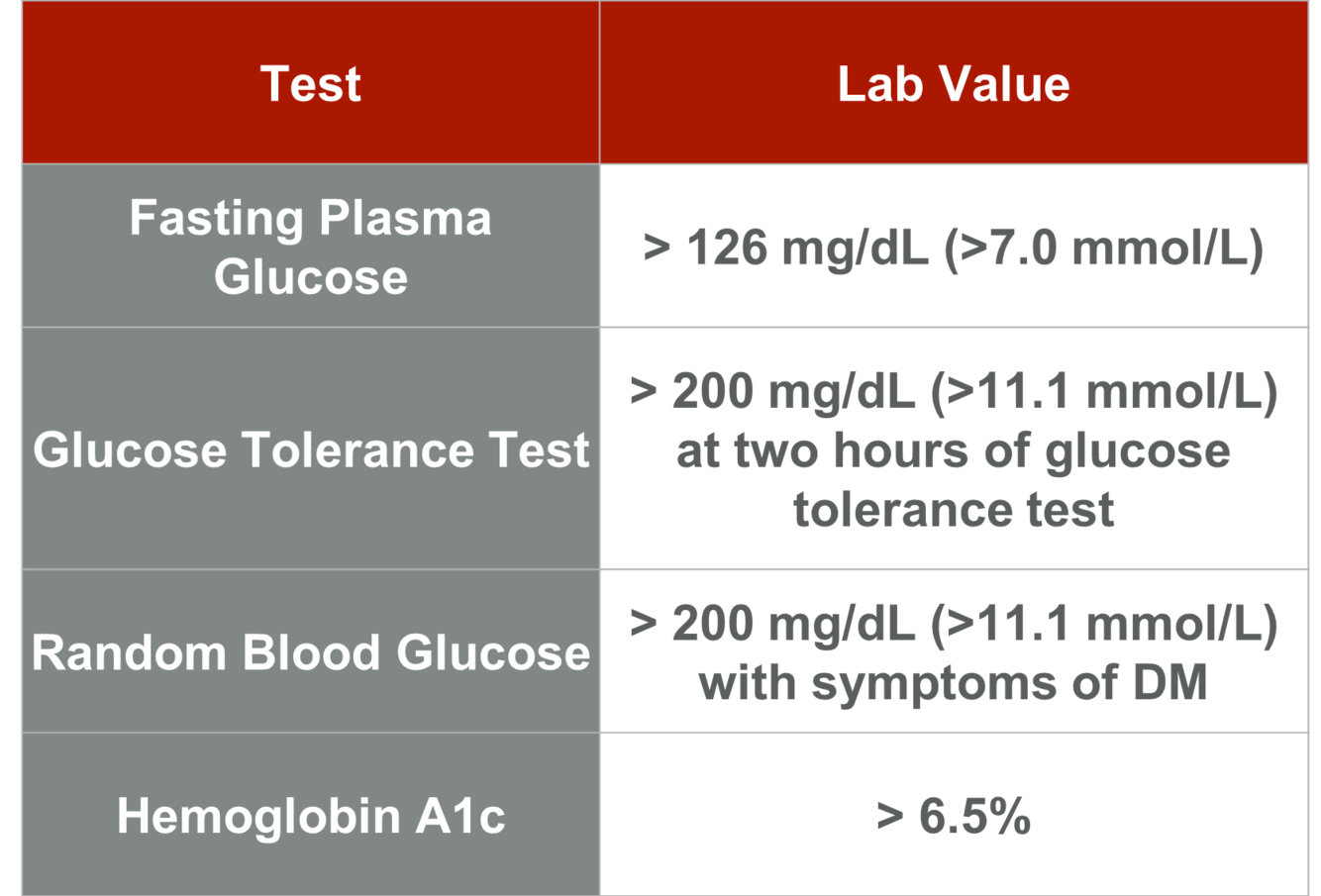
Diabetes mellitus diagnosing
If someone has a hmoglobin A1c greater than 6.5% they have DIABETES
Type I diabetes mellitus
REQUIRE TX WITH INSULIN DUE TO INSULIN DEFICIENCY
- Basal/bolus (most common)
–> once or twice daily long-acting insulin inject
–> short-acting insulin bolus for meals/snacks
- Continuous infusion
–> aka insulin pump, continuous infusion of short-insulin
–> bolus of short-acting insulin with meals
- Split/mixed
–> multipe daily injections of combination of long and short acting insulin (generaly worse glycemic control, more hypoglycemia)
Type II diabetes mellitus treatment
- Do not routinely require insulin at diagnosis
- many will eventually require insulin as the disease progresses
- choice therapy depends on severity of hyperglycemia, patient comfort, patient willingness
- typically will start with oral therapies and adjust as needed
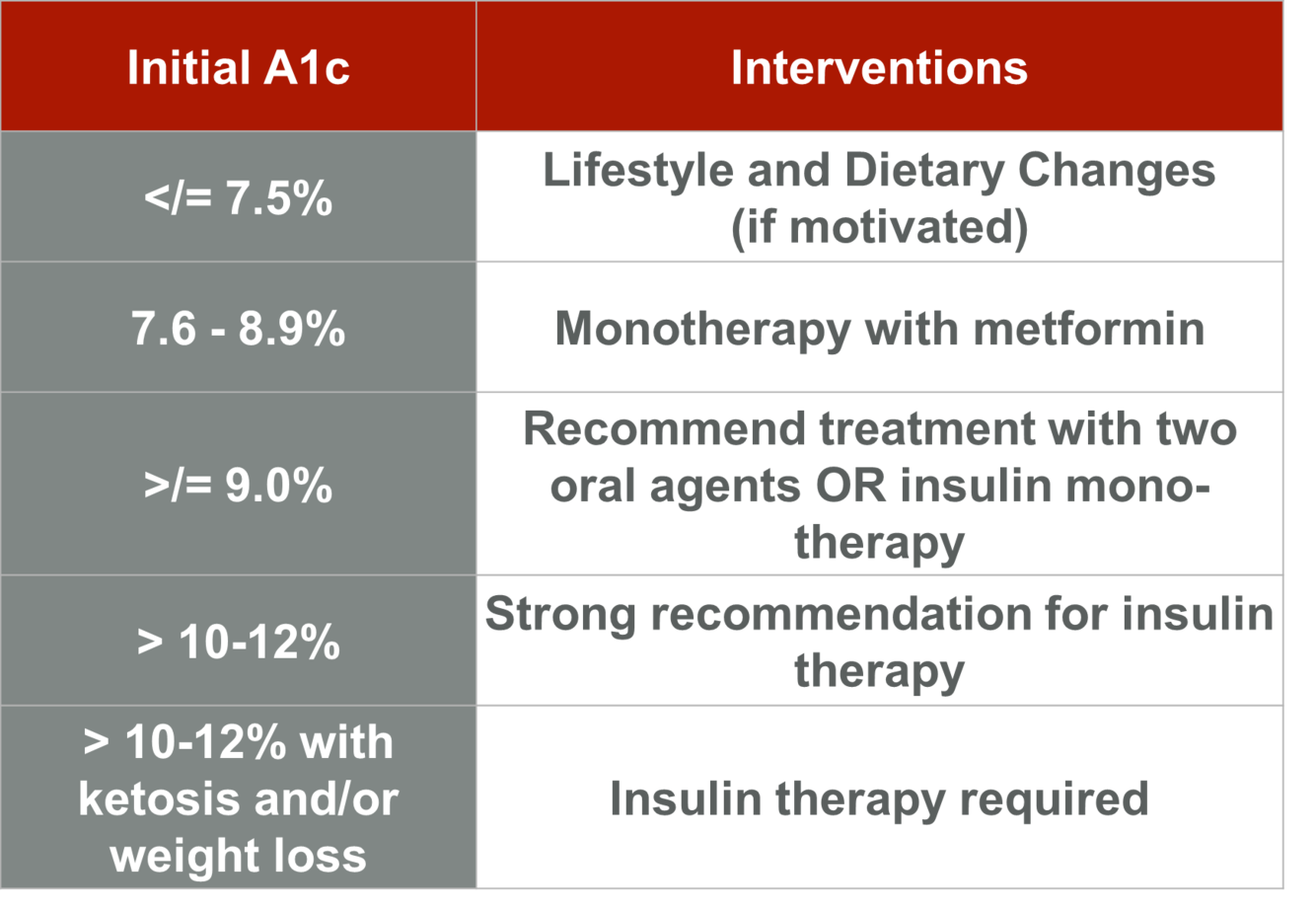
describe the treatment options for varying levels of initial A1c
- Meformin is the standard (7.5-9%)
>9 - two oral agens or insulin monotherapy
> 10-12% = strong recommendation for insulin therapy
> 10-12% with ketosis and or weight loss = insulin therapy required
describe diet and lifestyle changes
- ADA recommends 150 minutes/weeks of moderate intensity cardio workouts
–> 3x/wk, no more than 2 days off in between
- recommends resistance training at least twice per week
- HYPO-CALORIC with LOW FAT or LOW CARBO intake
–> consistent carbohydrate intake, recommend 45-65% of total daily calories
**WEIGHT LOSS IS MORE IMPORTANT THAN CERTAIN COMBINATIONS OF NUTRIENTS**
METFORMIN
- Decreases hepatic gluconeogensis and glucogenolysis with increase in peripheral insulin sensitivity and glucose uptake
- SIDE EFFECTS = diarrhea, indigestion (resovle within weeks), LACTIC ACIDOSIS
- CONTRAINdiCATIONS
–> renal or hepatic impairment (Cr > 1.5 mg/Dl in men or Cr > 1.4 inw omen) –> DO NOT USE
–> binge drinking, cirrhosis or use a radio contrast dye
–> predisposition for LACTIC ACIDOSIS (CHF or chornic hypoxemia)
describe Metformin dosing
- Initial mono-therapy when single agent is used
- Start dosing at 500mg once or twice daily with meals
- If patient continues to tolerate medication, double dose every 5-7 days until at goal of 1000mg twice daily (GOAL TX)
- this should not be used in women who are PREGNANT or MAY BECOME PREGNANT
Sulfonylureas
- Stimulate insulin secretion by pancreas beta cells
- Decrease the microvascular complications of diabetes
- ASE: weight gain, hypoglycemia, increased CV events
- Decrease efficacy with time, therefore will need increasing dose
Thiazolidinediones
- act on receptor in muscle, fat and liver to sensitize them to insulin (PPAR gama gene)
- Less effective than sulfonyurea, metformin
- increased risk of fluid retention and CHF; contraindicated in NTHA class III or IV
- reported increased risk of bladder cancer with > 1 year of use
Glitinides
- similar to sulfonylureas, stimulate beta cells
Alpha-glucosidase inhibitors (Acarbose)
- prevent absorption of simple sugars by decreasing carbohydrate breakdown
- less effective but less wieght gain
DPP-4 inhibitors (sitagliptin)
- DDP-4 degrades incretin (which stimulates insulin secretion)
- increased incretin leads to increase insulin secretion
- Few ASE: pancreatitis, angioedema, urticaria
GLP-1 Receptor antagonist (exanatide)
- Increase insulin and decrease glucagon, increase anxiety
- no hypoglycemia, causes weight LOSS
- ASE: increase hypoglycema with combination, pancreatitis
Sodium-glucose co-transport 2 (SGL T2) inhibitors (canagliflozin)
- newest class, block glucose reabsorption in the kidney
- less hypoglycemia, causes weight loss
- ASE: dehydration (glucosuria), fungal genital infections
- Do not use in Chronic kidney disease
Insulin therapy (type II) dosing
- MOST EFFECTIVE medication to lower A1c
- typically Start with long-acting insulin ONCE DAILY
–> 0.1-0.2 Units/kg initially –> 10 units minimum
–> monitor daily morning fasting glucose and titrate insulin until goal of 70-130mg/dl
- Initial goal of insulin therapy is to obtain fasting glucose levels less than 130 mg/dL in the morning
–> if A1c is still not in range after 3 months add MEALTIME SHORT-ACTING INSULIN (designed to mimic insulin production by the pancreas)
What are the glycemia treatment goals
- A1c =
- Preprandial glucose (fasting) = 70-130 mg/dL
- peak postprandial glucose =
What types of annual screening: ***
- Spot urine albumin-to-creatinine ratio (normal < 30 mg/g)
–> if > 30mg/g, recheck to confirm
- foot exam with monofilament testing
–> assess loss of protective sensation
–> check for pulses, ulcers, nail pathology
- Dilated eye exam by ophthalmologist
–> monitor for diabetic retinopathy
