EACDIT of Carcinoid Syndrome
E: Rare.
A: Neuroendocrine tumour; secretes serotonin, histamine and bradykinin. Slow-growing. Commonly metastasizes to liver. Must be present in liver for symptoms.
C: Diarrhoea, SOB (bronchoconstriction due to serotonin), Flushing (Histamine/Bradykinin) & Pruritus. Pellagra (reduced tryptophan; niacin). Tricuspid regurg & pulmonary stenosis (serotonin causes fibrosis).
DDx: Serotonin Syndrome
Ix: Oscreotide Scan, Urinary 5-Hydorxyindoleacetic acid (5-HIAA) & Niacin. Plasma Chromogranin Ay (statin)
Tx: Somatostatin analogues (inhibitory); Ocreotide, Chemo & Lifestyle: reduce stress and alcohol. Surgical resection. Cyproheptadine for diarrhoea.
Pellagra features
Niacin (B3) defiency
The 3 D’s
Diarrhoea
Dermatitis
Dementia
(Multiple Endocrine Neoplasia) MEN I EACDIT
E: Autosomal Dominant mutation in MEN1 gene (tumour suppressor) on Chromosome 11.
A: affects the Pituitary (adenoma), Parathyroid (95%) & Pancreas (3 P’s). Most common is parathyroid - hyperparathyroidism (increased calcium), early age (25yrs) and affects multiple glands.
C: Headaches/Bitemporal hemianopia/Diplopia (pituitary adenoma). Hypercalcaemia (bones, stones, groans, psychic moans), Peptic Ulcers (gastrinoma aka Zollinger-Ellison), Insulinoma (hypoglycaemia), Glucagonoma (hyperglycaemia). Adenomas (prolactinoma): Galactorrhea/Gynaecomastia. Acromegaly/Gigantism.
Dx: Clinical findings.
Ix: Genetic testing.
Tx: Parathyroidectomy. Pituitary - surgical if ACTH or dopamine agonist (ropinirole) if prolactinoma.
(Multiple Endocrine Neoplasia) MEN IIa EACDIT
E: Autosomal Dominant mutation in RET gene (proto oncogene) on chromosome 10.
A: affects the Parathyroid, Medullary (C-cells secrete calcitonin) Thyroid & Phaeochormocytoma (epinephrine/norepinephrine)
C: Anxiety, sweating, HT. Hoarseness, coughing and dysphagia (Thyroid).
Dx: Clinical findings.
Ix: Genetic testing
Tx: Surgery; thyroidectomy
(Multiple Endocrine Neoplasia) MEN IIb EACDIT
E: Autosomal Dominant mutation in RET gene (proto oncogene) on chromosome 10.
A: affects the Mucosa (skin and mouth), Marfan, Medullary Thyroid & Phaeochromocytoma (4 M’s). Multiple neuromas (nerve tissue).
C: Hoarseness, coughing and dysphagia (Thyroid).
Dx: Clinical.
Ix: Genetic testing. Urinary metanephrines.
Tx: Surgery; thyroidectomy.
Cushing’s Syndrome
A: Excessive cortisol.
Exogenous (more common): long-term steroid use
Endogenous (less common): Pituitary adenoma (Cushing’s disease); secretes ACTH or Ectopic (small cell lung Ca)
Ix: Overnight Dexamethasone suppression test.
Low dose (1mg) suppression: indicates exogenous cause (steroids)
High dose (8mg) suppression: indicates endogenous (pituitary; if cortisol suppressed also). Cortisol unaffected; adrenal adenoma.
No suppression: indicates paraneoplastic (ectopic) secretion (i.e. small cell lung Ca or carcinoid; less common)

Primary Hyperaldosteronism (Conn’s Syndrome)
Aetiology: Increased aldosterone (mineralocorticoid; increased Na reabsorption & increased K/H secretion).
Causes: Bilateral idiopathic adrenal hyperplasia (70%; commonest cause). Adrenal adenoma (unilateral). Familial hyperaldosteronism. Adrenal carcinoma (rare).
Signs: HT, Hypokalaemia, alkalosis
Symptoms: Muscle weakness
Ix: Aldosterone:Renin ratio; High:Low (due to high BP). High-res CT; adrenal venous sampling to distinguish between bilateral/unilateral if CT is negative.
Tx: Adrenal adenoma (surgery). Bilateral adrenocortical hyperplasia (spirinolactone; aldosterone antagonist)
Secondary Hyperaldosteronism
Aetiology: Increased renin. Renal BP is lower vs. systemic BP. Causes: RAS (atherosclerosis), Renal Artery obstruction, HF.
Clinical Features: HT (tx-resistant), hypokalaemia, alkalosis, muscle weakness.
Ix: Aldosterone:Renin ratio: High:High. Doppler US (RAS). BP. U&Es (hypokalaemia). Alkalosis.
Imaging: CT/MRI (adrenal tumour). Doppler/CT Angio/MRA (RAS, Obstruction).
Tx: Aldosterone antagonists (eplerenone/spironolactone). Surgery (adenoma). Percutaneous renal artery angioplasty (RAS).
Prolactin and galactorrhoea
Aetiology: Prolactin is secreted by the Ant. Pituitary. Dopamine inhibits prolactin relaease.
Causes: P’s
- Pregnancy
- Prolactinoma
- Physiological - stress, exercise, sleep
- Polycystic ovarian syndrome (PCOS)
- Primary hypothyroidism (TRH)
- Phenothiazines (chlorpromazine), metoclopramide, domperidone, haloperidol
Clinical Features:
Men; impotence, low libido, galactorrhoea.
Women; amenorrhoea, galactorrhoea.
Tx: Dopamine antagonists (bromocriptine)
Thyroid Cancers
Types (by prevalence):
Papillary (3 P’s: Prognosis good, Psamomma bodies (pale empty nuclei), Prevalent): Young females.
Follicular: Solitary nodule.
Medullary: Parafollicular C-cells; secrete calcitonin (low PTH); part of MEN-II. Endocrine features of Skin flushing (Serotonin) & Diarrhoea (VIP).
Anaplastic: Non-responsive to Tx. Elderly females. Aggressive.
Clinical Features: Solitary painless nodule. Firm and non-mobile. Hoarseness. Dysphagia. Non-functional (no signs of thyroidism).
Ixs: US of thyroid gland. FNA.
Treatment (papillary/follicular): Total thyroidectomy + radioiodine (I-131). Yearly thyroglobin levels (disease recurrence).
Primary Adrenal Insufficiency (Addison’s)
E:
A: Autoimmune destruction of adrenal cortex (developed countries). Reduced cortisol and aldosterone (destruction of adrenal cortex).
Primary causes
- TB (developing countries; spreads to adernal cortex)
- Metastases (e.g. bronchial carcinoma)
- Meningococcal septicaemia (Waterhouse-Friderichsen syndrome)
- HIV
- Antiphospholipid syndrome
Secondary causes
- pituitary disorders (e.g. tumours, irradiation, infiltration)
- Exogenous glucocorticoid therapy
C:
- lethargy, weakness, anorexia, N&V, wt loss, ‘salt-craving’
- Hyperpigmentation (primary; notably palmar creases), vitiligo, loss of pubic hair in women, hypotension, hypoglycaemia
- Hyponatraemia and hyperkalaemia
- Addisonian Crisis: collapse, shock, pyrexia
Ix: ACTH stimulation (Synacthen). Primary: High serum ACTH. Secondary: Low ACTH.
- Renin levels are typically high (stimulates aldosterone release) and aldosterone levels low in Addison’s disease.
- In secondary adrenal insufficiency, the renin-angiotensin system can function normally.
- Serum DHEA-S — typically low in Addison’s disease.
- Thyroid function tests.
- Autoantibody levels — adrenal cortex autoantibodies or antibodies against 21-hydroxylase are present in more than 80% of people with recent-onset autoimmune adrenalitis.
Tx: Hydrocortisone (glucocorticoid) & Fludrocortisone (mineralocorticoid). DHEA. Double hydrocortisone dose during illness, injury or surgery.
ADDISONIAN CRISIS: IM Hydrocortisone. Features may include hypotension, hypovolaemic shock, delirium, reduced consciousness, acute abdominal pain, vomiting, headache, low-grade fever, and muscle weakness.

Addisonian Crisis
Causes
- Sepsis or surgery causing an acute exacerbation of chronic insufficiency (Addison’s, Hypopituitarism)
- Adrenal haemorrhage eg Waterhouse-Friderichsen syndrome (fulminant meningococcemia)
- Steroid withdrawal
Management
- Hydrocortisone 100 mg IM or IV
- 1L NaCl infused over 30-60 mins or with dextrose if hypoglycaemic
- Continue hydrocortisone 6 hourly until the patient is stable. No fludrocortisone is required because high cortisol exerts weak mineralocorticoid action
- Oral replacement may begin after 24 hours and be reduced to maintenance over 3-4 days
Interpret the Thyroid results:
TSH 14.3 (05.-5.5)
Free T4 14 (9-18)
Poor Compliance with Thyroxine

TSH High
T4 Low
Interpret the Thyroid results:
TSH 3.4 (0.5-5.5)
Free T4 21.3 (9-18)
Thyrotoxicosis (e.g. Graves’ disease)
TSH Low
T4 High*
*In T3 thyrotoxicosis the free T4 will be normal
Interpret the Thyroid results:
TSH 7.2 (0.5-5.5)
Free T4 4.3 (9-18)
Primary hypothyroidism
TSH High
T4 Low

Interpret the Thyroid results:
TSH 0.2 (0.5-5.5)
Free T4 3.7 (9-18)
Secondary hypothyroidism
TSH Low
T4 Low
Replacement steroid therapy is required prior to thyroxine

Interpret the Thyroid results:
TSH 0.1 (0.5-5.5)
Free T4 3.9 (9-18)
Sick euthyroid syndrome
TSH Low
T4 Low
Common in hospital inpatients
T3 is particularly low in these patients

Interpret the Thyroid results:
TSH 7.6 (0.5-5.5)
Free T4 11.3 (9-18)
Subclinical hypothyroidism
TSH High
T4 Normal

Interpret the Thyroid results:
TSH 0.2 (0.5-5.5)
Free T4 12.9 (9-18)
Steroid therapy
TSH Low
T4 Normal

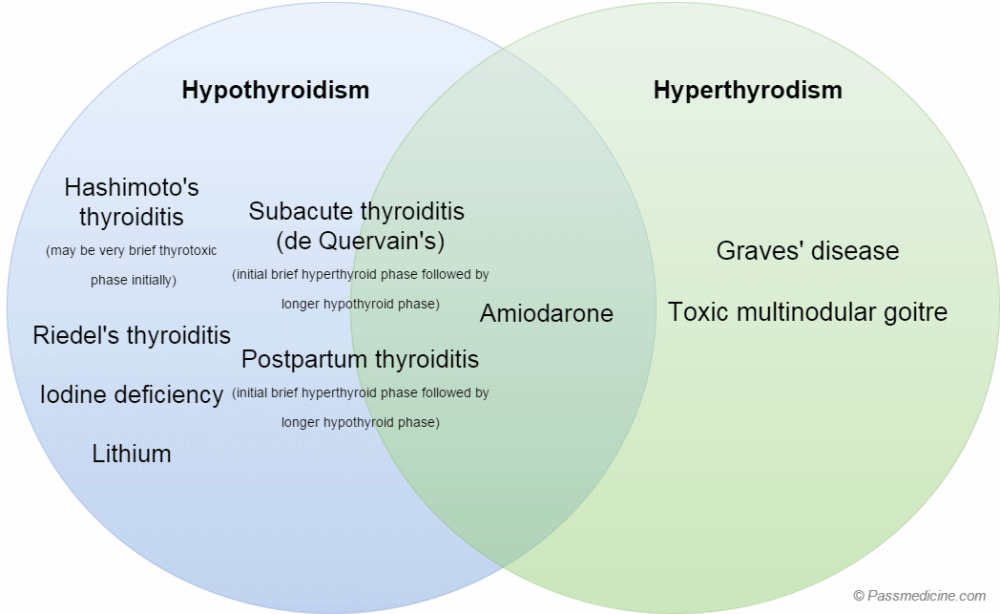
Thyroidism Causes
Hypothyroidism
Hyperthyroidism
Grave’s Disease
E: 30-40yrs. F:M (8:1). FHx. Smoking.
A: Autoimmune. 80% genetic. IgG Abs to TSH Rs; cause chronic stimulation.
C: Heat intolerance, wt loss, sweating, palpitations, tachycardia, anxiety, tremor. Eye disease: exophthalmos. Pretibial myxoedema: waxy discolouration of shins.
Ix: TFTs: TSH low, T3/4 High. Specific test: TSH R. Abs (TRAbs). Technetium scan of thyroid gland: considered if TRAbs are negative.
Tx:
ß-blockers (Symptom-control)
- For rapid control of hyperthyroidism symptoms, including palpitations, tachycardia, anxiety, and heat intolerance. E.g. propranolol.
Radioactive iodine:
- 1st line definitive treatment, unless antithyroid drugs are likely to achieve remission or it is unsuitable. It may be unsuitable due to pregnancy, attempts to conceive within the next 4-6 months, presence of active eye disease, or concerns about compression or malignancy.
- Patients often become hypothyroid, thus may require replacement therapy.
Antithyroid drugs
- Offer a 12-18 month course as first-line definitive treatment if it is likely to achieve remission, or if radioactive iodine and surgery are unsuitable.
- Remission is the continuation of euthyroid status after withdrawal of antithyroid drugs and occurs in around 50% of Graves’ patients. Remission is more likely in mild and uncomplicated Graves’ disease.
- Examples include carbimazole (first-line) and propylthiouracil.
Surgery
- Total thyroidectomy offered as first-line definitive treatment if concerns about compression or malignancy, or radioactive iodine and antithyroid drugs unsuitable.
- Consider if antithyroid drugs have been tried but hyperthyroidism persisted or relapsed.
- Risks: recurrent laryngeal nerve damage, hypoparathyroidism.
- Patients become hypothyroid, thus require replacement therapy.
When to avoid radioactive Iodine
Important exceptions to using radioactive iodine first-line include:
- Pregnancy
- Attempts to conceive within the next 4-6 months
- Presence of active eye disease
- Concerns about compression or malignancy.
- In these cases, it must be considered whether surgery or antithyroid drug therapy is the most appropriate option.
Hypothyroidism
E: 5-10x more common in females.
A: Hashimoto’s thyroiditis (developed). Iodine deficiency (developing). Iatrogenic (surgery, medications - lithium, amiodarone).
Secondary causes (rare): Hypopituitarism (TSH impaired); tumours, infection, vascular (sheehan’s) and radiation.
C: Weight gain, fatigue, Cold intolerance (sensitive to cold), fatigue, ammenorrhoea, constipation, fluid retention. Deep tendon reflexes. Hoarse voice. Dry, coarse scalp hair, loss of lateral aspect of eyebrows
Ixs: TSH, TFTs: Primary Hypothyroidism:TSH High & TFTs Low(no negative feedback).Secondary Hypothyroidism:TSH & TFTs Low.
Specific tests: Thyroid peroxidase antibody (TPOAb) & Thyroglobulin antibody (TgAb)
Tx: Oral levothyroxine (synthetic T4). Measured monthly until stable (TSH high indicates low dosage. TSH low indicates high dosage).
Subacute Thyroiditis
E: 20-30yrs. F:M (4:1)
A:
C: Initial Hyperthyroid followed by prologonged Hypothyroid phase.
- phase 1 (lasts 3-6 weeks): hyperthyroidism, painful goitre, raised ESR
- phase 2 (1-3 weeks): euthyroid
- phase 3 (weeks - months): hypothyroidism
- phase 4: thyroid structure and function goes back to normal
Ix: Thyroid scintigraphy: globally reduced uptake of iodine-131
Tx:
- usually self-limiting - most patients do not require treatment
- thyroid pain may respond to aspirin or other NSAIDs
- in more severe cases steroids are used, particularly if hypothyroidism develops
-
Cardiology90
-
Emergency8
-
Neurology19
-
Respiratory18
-
Ophthalmology79
-
Endocrine30
-
Reproductive Medicine39
-
Obstetrics & Gynaecology91
-
Infectious Diseases1
-
Surgery79
-
Ethics & Law0
-
Therapeutics76
-
ENT64
-
Psychiatry96
-
Dermatology76
-
Acute Medicine87
-
Paeds80
-
Haematology67
-
Renal Medicine87
-
Clinical Anatomy59
-
Clinical Imaging2
