What are the indications for obtaining a KUB?
How is it obtained?
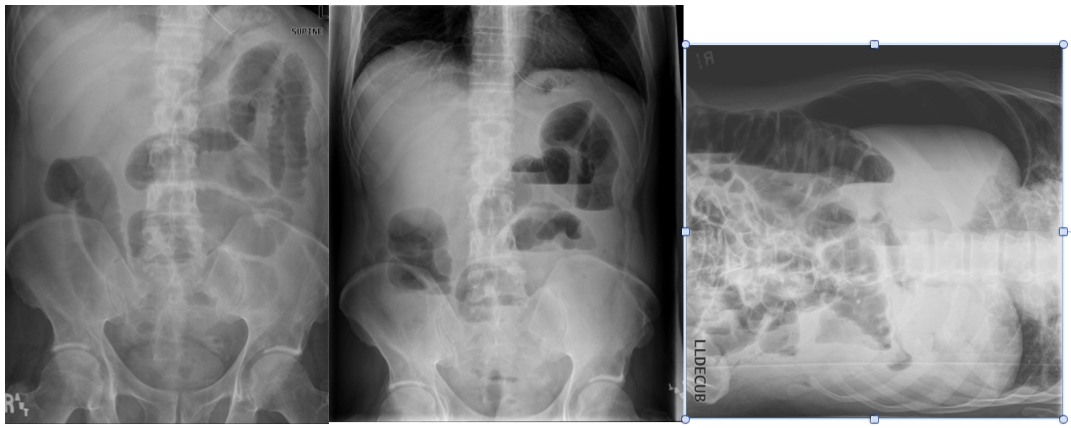
Abdominal pain
supine + upright (if a patient can’t stand upright, then get a lateral decubitus instead)
obtained on an empty stomach (if bowel is filled with fluid, then it won’t show up on the radiograph)
What are the indications for obtaining a fluoroscopy?
What contrasts are employed?
Pain, dysphagia, diarrhea, hernias, colon cancer
Double contrast-air and barium - mucosal detail
Single contrast-barium only - peristalsis, wall, folds, caliber

What are the indications for obtaining a CT?
How is it obtained? What contrasts are employed?
Abdominal pain, Bowel pathology, Tumors, Weight loss, vague symptoms
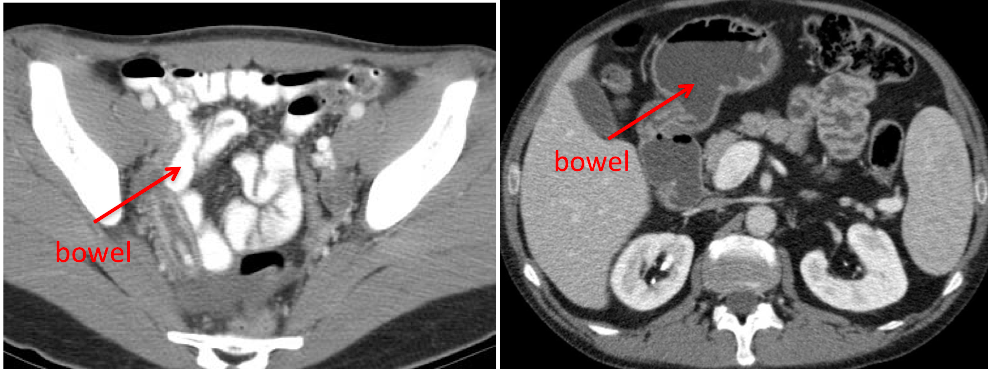
Positive (high density) oral contrast – differentiate between fluid collections (ie abscess) from bowel.
Negative (low density) oral Contrast (H: evaluate bowel mucosa and wall better
Timing of scan depends on the organ of interest and the pathology (hypervascular vs hypovascular), but involves some sort of scan delay (time from contrast injection to starting the scan).
- the liver has a predictable peak attenuation at 60 seconds
- these multiple phase studies are avoided in younger patients due to radiation risks!
What are the indications for obtaining a MRI?
- when CT is indeterminate - abd imaging in young patients (no radiation) - Iodine allergy - Crohn disease (MR enterography-study of small bowel) - Hepatobiliary imaging (MRCP) –obstruction of common bile duct - Tumors, masses
What are the indications for obtaining a US?
obstruction of the cystic duct (cholelithiasis, acute cholecystitis)
What are the indications for obtaining a nuclear medicine scan?
bile leaks, cystic duct obstruction
What is Inflammation?
What type of imaging would you use and not use?
How is solid organs, fat, and bowel wall affected with inflammation on a CT scan?
Inflammation: Accumulation of fluid and inflammatory cells as a result of increased vascular permeability (results in swelling) and vascular dilation (allows for hyper-enhancement with IV contrast.
- *Radiography**
- Organ inflammation - usually occult or non-specific (ex hepatomegaly)
- May see mass effect on gas filled loops of bowel from adjacent inflammation
- *CT +/- IV contrast**
- fast sensitive
- *US**
- can’t see through fat because it’s echogenic – sound beam hits fat and bounces back to the sensor (therefore anything behind the fat is not seen!)
- *MRI**
- very good, but very costly and long exam time
Solid organs – density will decrease with inflammation (organs are denser than fluid); likely also see organomeagly
Fat – density will increase (fluid is denser than fat); will see fat stranding (fine or smudgy strands of hazy density)
Bowel wall – no appreciable change in density with inflammation of the wall (although it may be thicker and effaced), but will see mucosal hyper-enhancement (due to hyperemia)
What is the normal size of bowel wall (small + large) on imaging?
What causes the thickness of the bowel wall to change?
What type of imaging would you use and not use?
What is a unique finding on bowel walls on imaging?
Normal
- Small bowel: 1.5mm thick
- Colon: 3mm thick
thickness changes with inflammation, infection, hemorrhage, neoplasm, infiltration, or ischemia
- *Radiography**
- thickness - only seen if bowel is filled with air
- not sensitive or specific
- *CT**
- sensitive +/- specific
- provides greater detail about fold patterns, adjacent mesentery, LN, or mesenteric masses; inflammation (mucosal enhancement stranding, etc) or neoplastic infiltrations
- *Fluoroscopy**
- can show luminal narrowing or effacement, BUT it does not show the vascular dilatation, mucosal hyperenhancement, or degree of wall thickening.
- *MRI**
- Sensitive, but too costly and long acquisition time (peristalsis can cause motion effects on the image; solution: administer glucagon to decrease peristalsis)
- *US**
- cannot evaluate an air-filled bowel
- *Thumbprinting**
- occurs due to ulcerations with heaped up, edematous mucosa, resulting in small areas of increased radiographic density “someone is taking their thumb and pushing it from the outside in”
- seen better with contrast
- common in Crohns and infectious colitis (ie pseudomembrane colitis)

What are the various types of solid organ masses are observed with imaging?
What type of imaging would you use and not use?
How does imaging change with cysts? tumors?
Benign or malignant masses that can be
- focal mass
- infiltrative
- hypervascular (lots of angiogenesis)
- hypovascular
- *Radiography & fluoroscopy**
- masses are usually not identifiable unless they cause organomeagly or displacement of bowel loops
- *CT**
- sensitive - masses are visible with contrast if the difference in attenuation between the mass and normal organ parenchyma is large enough
- must acquire image at appropriate time otherwise the contrast will be “washed out” – point where the attenuation in the tumor and normal parenchyma will catch up together and be difficult to observe
- *MRI w. contrast**
- sensitive, but $$$$
- *US**
- very subtle; not sensitive
Cysts
- fulid filled sacs that can occur on any solid organ, but is most common in the liver, kidney, and pancreas. Low density on CT (water has 0 HU)
Tumors
- hypovascular - enhance less avidly
- hypervascular - enhances more avidly
How does tumor vascularity (hypo-/hyper-) affect image acquisition?
When would you acquire imaging for each one?
Bonus: give an example of each one
- *Hypovascular masses**
- enhance less avidly than the organ; mass is lower in attenuation than adjacent enhanced organ
- acquire the image at the time of peak organ enhancement
- example: colonic adenocarcinoma metz
Hypervascular masses
- enhance more avidly and rapidly than the organ; higher in attenuation than the organ
- acquire image at the time of peak tumor enhancement
- example: primary hepatocellular carcinoma
What is an obstruction?
What is the normal bowel diameter?
What type of imaging would you use and not use? (what are some features to each)?
What do you see upstream of the obstruction? downstream?
Blockage of flow of fluid or air within a lumen channel (can happen anywhere in the GI, biliary system, pancreatic duct, etc); numerous etiologies (strictures, adhesions, stones)
Normal small bowel diameter: < 2.5cm transverse diameter
- *Radiography**
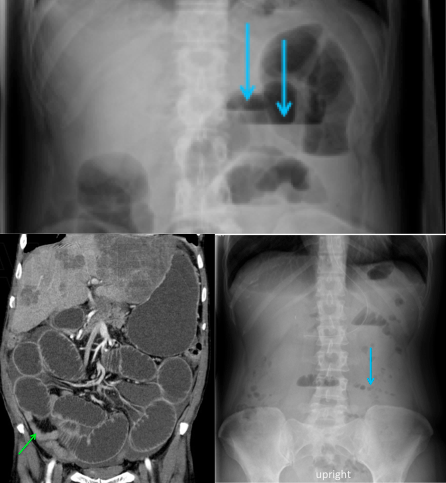
- can see dilated bowel loops (>3cm) with air fluid levels (mucosa continues to secrete fluid despite obstruction and shows up at the same density as solid masses/organs)
- *CT**
- obstruction can show up as decompression of normal small bowel or colon; greater details
- stones can allow visualization of ductal dilation as well as causes of ductal obstruction (but not stones)
- *MRI**
- evaluate ductal dilation + causes of ductal obstruction (including stones), but $$$$
Upstream of obstruction - lumen dilates; usually presence of air-fluid levels (may show up as a string of pearls sign (air trapped in plica circularis))
Downstream of obstruction – lumen decompresses as normal flow of fluid/air evacuates the lumen distal to the obstruction
What is an Ileus? What are the common causes of ileus?
What type of imaging would you use and not use? (what are some features to each)?
What do you see on a supine image? upright image?
Absence of normal bowel peristalsis, results in decreased antegrade movement of intestinal contents; caused by:
- post-op, Rx, etc
- adjacent inflammation can cause focal ileus (ie acute appendicitis)
Use Radiography or CT
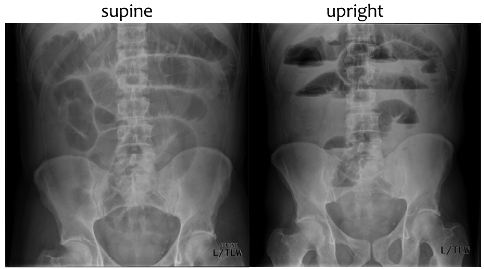
- Progressive dilation of small and large bowel
- Presence of air fluid levels in small bowel and colon (can only be seen on upright and lateral decubitus (not on supine)
Supine - Dilated small & large bowel on supine image
Upright - Air fluid levels in small & large bowels and colon (can only be seen on upright and lateral decubitus (not on supine))
-
11a. Pancreatic Function (Camtasia)32
-
6. Pathology of Mouth & Esophagus80
-
10. Disorders of GB and Biliary Tract81
-
9. Conf 1: GERD, Pelv Ulcer Dz, Esop Cancer40
-
11b. Pancreatitis: Acute and Chronic26
-
11c. Clinical Aspects of Acute and Chronic Pancreatitis43
-
7. Pathology of Gastric Diseases90
-
8. Path Lab: Upper GI19
-
12. Pancreatic Carcinoma42
-
13. Path Lab: Pancreas and Gallbladder30
-
GI Imaging12
-
Enteric Nervous System & Motility d/o53
-
Diarrhea25
-
Diverticular Diseases and Appendicitis15
-
22a. IBD Preview50
-
23. IBD Treatment and Risk/Benefit21
-
22b. IBD Interactive Session25
-
Liver Structure & Function48
-
Viral Hepatitis65
-
Advanced Liver Disease (Cirrhosis)56
-
25. Conference 337
-
26. Tumors of the Bowel78
-
27a. Maldigestion, Malabsorption CAMTASIA45
-
27b. Maldigestion, Malabsorption29
-
32. Pathology of Hepatitis53
-
33. Path Lab: Inflam and Neoplastic Dz of Bowel39
-
34. Alcoholic Liver Dz, Non-alc Fatty Liver44
-
35. Metabolic/Storage Dz of Liver60
-
36. Pathogenesis of Cirrhosis/Liver Tumors29
-
37. Autoimmunity and the Liver35
-
38. Conference 526
-
39. Integrated Response to a Meal0
-
40. Conference #6 (Surgery)1
-
41. Conference #70
-
42. The Tail End of Things30
-
43. Pediatric GI27
-
1 & 2. Esophageal Physiology & GERD36
-
3a. Gastric Acid Secretion CAMTASIA48
-
3b. Gastric Acid Secretion Interactive4
-
4. Peptic Ulcer Disease11
-
Conference #220
