Anemias
- Divide based on size of the red blood cell. MCV tells you this!
- Mean corpuscular volume (MCV) The average volume of red blood cells (RBC), calculated from the hematocrit (Hct) and the RBC count, in RBC indices.
- The calculation is: MCV = Hct × 10 ÷ RBC.
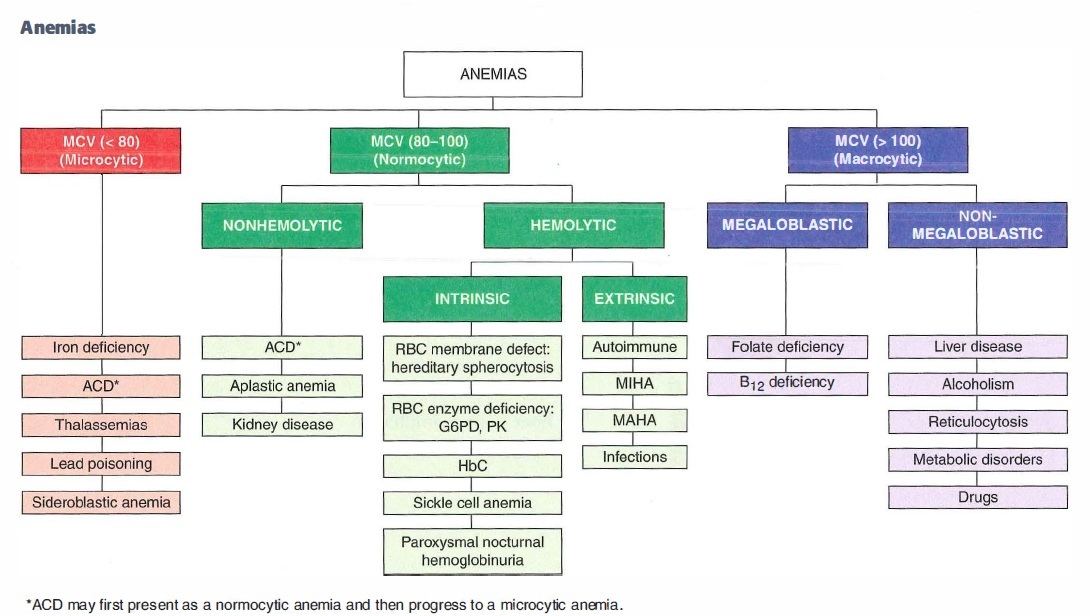
Microcytic, hypochromic (MCV <80)
- Iron deficiency
- ACD
- Thalassemias
- Lead poisoning
- Sideroblastic anemia
Normocytic, normochromic anemia
NONHEMOLYTIC
- ACD
- Aplastic anemia
- Kidney disease
HEMOLYTIC: Intrinsic and Extrinsic
**Intrinsic **
- RBC membrane defect: hereditary spherocytosis
- RBC enzyme deficiency: G6PD, PK
- HBC
- SCA
- PNH
Extrinsic
- Autoimmune
- MIHA
- MAHA
- Infections
Macrocytic anemia (MCV >100)
MEGALOBLASTIC
- Folate deficiency
- B12 deficiency
NON-MEGALOBLASTIC
- Liver disease
- Alcoholism
- Reticulocytosis
- Metabolic disorders
- Drugs
TIBC
total iron binding capacity = transferrin x 1.4. Anything that elevates transferrin will elevate TIBC
Ferritin
Ferritin is an acute phase reactant and is elevated in any type of inflammatory processes: Infection, cancer.
Stored iron inside cells. In Iron deficiency, you’ve used up all of the iron so ferritin stores will be low. In Anemia of chronic disease, ferritin stores are high.
Differentiating Iron deficiency vs Chronic disease
hang your hat on % transferrin saturation (Serum Fe/TIBC).
In Iron deficiency, your transferrin saturation will be markedly decreased b/c you have a lot of transferrin out there but little iron. Usually < 12% with Iron Deficinecy.
For chronic disease, it will either be normal or elevated usually >18, but anywhere from 12-45.
Hemochromatosis
Too much iron, transferrin is saturated, body is not making a lot of transferrin.
If normal ferritin, you can almost rule out hemochromatosis.
Elevated ferritin doesn’t prove hemochromatosis b/c it can be elevated for many reasons, it’s an acute phase reactant.
Lab findings that allow you to distinguish iron deficiency anemia from a microcytic, hypochromic anemia resulting from thalassemia
Iron deficiency will have
- ↓ Serum iron
- ↑TIBC ( a lot of transferrin)
- ↓ Ferritin
Thalassemia will have
- normal iron
- normal TIBC
- Normal ferritin
- target cells.
Megaloblastic anemia
Any anemia in which there is a predominant number of megaloblastic erythroblasts, and relatively few normoblasts, among the hyperplastic erythroid cells in the bone marrow (as in pernicious anemia).
Cell cycle cannot progress from G2 to M stage, and continued growth without division presenting as macrocytosis.
Megaloblasts - dysfuncitonal RBCs in bone marrow
Bone marrow filled with adipocytes
Aplastic anemia
Anemia + hypersegmented neutrophils + Neurological symptoms
B12 Deficinecy
Causes of aplastic anemia
“AA -> RV FIne” Failure or destruction of myeloid stem cells due to:
- RADIATION; drugs (Benzene, Chloramphenicol, Alkylating agents, Antimetabolites);
- Viral agents (parvovirus B19, EBV, HIV, HCV);
- Fanconi’s anemia (DNA repair defect);
- Idiopathic (Immune mediated, primary stem cell defect); may follow acute hepatitis.
“why take flight on AA when the RV is FIne”
Converts Vitamin K to activated vitamin K?
Effect of activated vitamin K?
- Epoxide reductase
- Acts as cofactor for II, VII, IX, X, C, S to help coagulate
Anti-coagulation
- Antithrombin inactivates factors II, VII, IX, X, XI, XII
- Protein C -> activated by thrombomodulin in endothelial cells to activated protein C (APC) -> Protein S acts on which cleaves and inactivates Va, VIIIa
- Plasminogen is activated by tPA to plasmin -> cleaveage of fibrin mesh
PT
PTT
PT - tests extrinsic (Tissue factor pathway) - I, II, V, VII, X
PTT - tests all factors except VII and XIII (intrinsic)
Most common hereditary thrombosis syndrome leading to hypercoagulability?
**Factor V Leiden **
- Most common cause of inherited hypercoagulability, 45-50% of all hypercoagulable states
- Production of mutant factor V - cannot be degraded by protein C
- Factor V is an accelerating factor that helps factor X convert prothrombin to thrombin (factor 5 is normally inhibited by protein C
2 most common inherited hypercoagulability disorder
Prothrombin gene mutation
- Prothrombin G20210A Mutation
- Mutation of Guanine (G) to Alanine (A) in 3’ untranslated region -> predisposes to thrombosis, associated with venous clots
- “Like 90210 except its 20210”
Effects of bradykinin
- ↑ vasodilation
- ↑ vascular permeability
- ↑ pain
Clinical consequence of deficiency in either protein C or protein S
- hypercoagulability and make too many blood clots
- (b/c C and S are anticoagulants, C can’t inactivate factors 5 and 8 which shut down clotting cascade.)
MOA of Heparin
- Supercharges antithrombin! (Antithrombin inactivates factors II, VII, IX, X, XI, XII)
- Cofactor for activation of antithrombin
- ↓ thrombin (thrombin converts fibrinogen to fibrin which is then activated by XIIIa to fibrin mesh)
- ↓ Xa (Xa converts prothrombin to thrombin)
- Short half-life
Clinical use of heparin
- Immediate anticoagulation for PE, stroke, Acute coronary syndrome, MI, DVT
- Used during pregnancy (does not cross placenta)
- Follow PTT
Toxicity of Heparin
Antidote for OD?
- Bleeding
- Thrombocytopenia (HIT)
- Osteoporosis
- Drug-drug interactions
- Rapid reversal - protamine sulfate (positively charged molecule that binds negatively charged heparin)
LMWH
Newer low-molecular-weight heparins
- Enoxaparin (Lovenox) acts more on Xa
- Dalteparin (newer) inactivates factor Xa (Xa converts prothrombin to thrombin)
- Better bioavailability
- 2-4 times longer half-life
- administered subcutaneously
- No laboratory monitoring - dosage based on weight
