Outline the blood supply to the uterus
Ovarian artery, from the abdominal aorta, supplies the fundus, uterine tubes and upper uterus.
The ovarian artery anastomoses with the uterine artery.
Uterine artery, from the internal iliac artery, supplies the remaining part of the uterus.
Vaginal artery, from the internal iliac artery, supplies the vagina.

Name the branches of the anterior and posterior divisions of the internal iliac artery
I Love Going Places In My Very Own Underwear
Iliolumbar
Lateral sacral
Gluteal (superior and inferior)
Pudendal (internal)
Inferior vesicle (vaginal in females)
Middle rectal
Vaginal
Obturator
Uterine
*First 3 branches orignate from the posterior division (superior gluteal only)

Outline the relations of the ovary
Posterior relations: Common iliac vein and artery, ureter
Lateral relations: Obturator nerve, artery and vein
Anterior superior relations: Obliterated umbilical artery (from the internal iliac artery, becomes the medial umbilical ligament)

Outline the blood supply and venous drainage of the ovary
Ovarian artery: Branches from the abdominal aorta
Uterine artery: Branch of the internal iliac artery. Forms an anastomoses with the ovarian artery
Paired ovarian veins drain the ovary.

Outline the lymphatic drainage of the ovary
Pre-aortic and para-aortic (sentinel node!) nodes.
Deep, not palpable
May also drain to superficial inguinal nodes
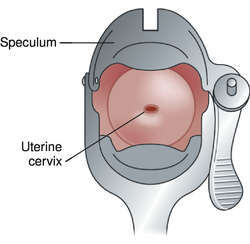
Describe the key features seen during speculum examination of the cervix and vagina
- External Os (ostium)
- Dome of the cervix
- Fornices (2 lateral, anterior and posterior)
NOTE: Nulliparous cervix is O like. Mutliparous cervix is inverted U shaped
Outline the autonomic and afferent innervation of the vagina
Autonomic supply
Upper 2/3rds: Receives sympathetic (T10-L2) and parasympathetic (S2-S4 pelvic splanchnics) supply via the hypogastric plexus
- Sympathetics from T10-L2 travel via superior hypogastric plexus. Split into R and L hypogastric nerves.
- The pelvic splanchnic nerves (S2-S4) join the (sympathetic) hypogastric nerves.
- Allows for the provision of autonomic sympathetic and parasympathetic supply to the vagina.
Lower 1/3rd: Receives sympathetic supply from the pudendal nerve (S2-S4), from the grey rami communicans, via the inferior rectal and perineal branches. NOTE does not have a parasympathetic supply.
Afferent
Upper 2/3rds: Travel back via the pelvic splanchnic nerves to S2,3 and 4. (REMEMBER THIS FOR REFERRED PAIN)
Lower 1/3rd: Travel back with the pudendal nerve, via the perineal branch, to S2-S4
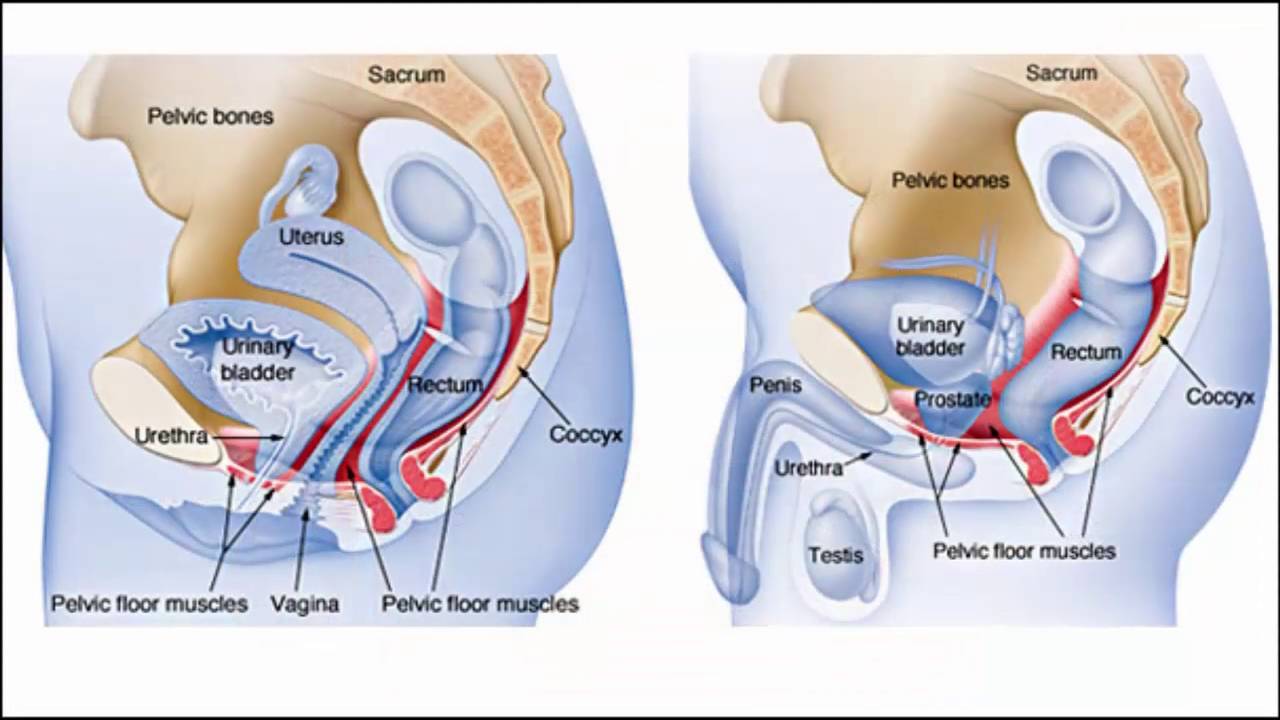
Describe the pelvic floor, perineal membrane and the perineal pouches, their relationship to each other and their contents in the male and female
- Outline the ‘layers’ of the area
- Pelvic floor: Muscular layer. Supports the pelvic and abdominal organs. Maintains continence.
- Perineal membrane: A covering of the urogential triangle. Continuous with the fascia covering the abdominal wall and the fascia lata of the thigh (preventing fluid spread in rupture)
- Perineal pouches: Deep and superficial.
Contents of the perineal pouches
Deep perineal pouch: Urethra, external utheral sphincter, vagina (females), bulbourethral glands and deep transverse peritoneal muscles (males)
Superficial perineal pouch: Erectile tissues (penis/clitoris), Bartholin’s glands, greater vestibular glands, 3 muscles (ischiocavernous, bulbospongiosus and superficial transverse perineal muscles), perineal body
Outline the fascia of the peritoneum
Scarpa’s (membranous) ▻ Dartos Fascia (penis) ▻ Colle’s fascia (urogenital triangle)
Camper’s (fatty) ▻ Dartos Muscle (scrotum)
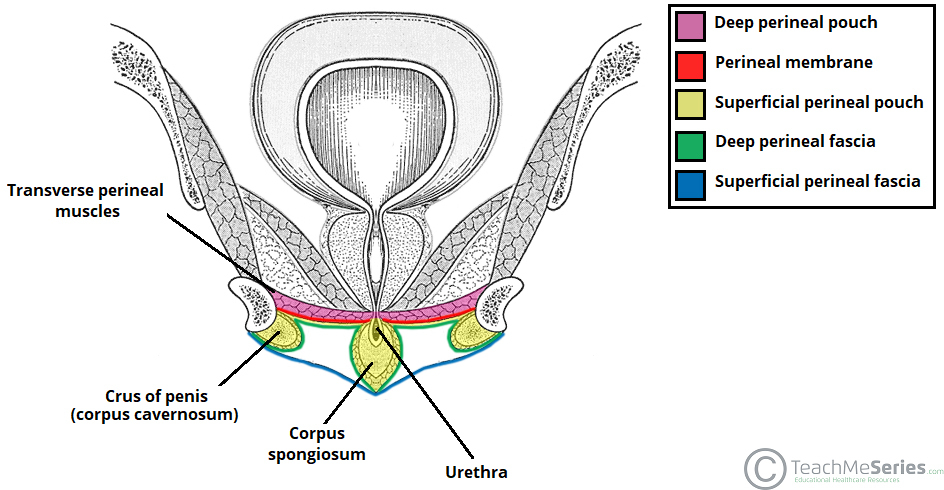
Outline the layers of the urogential triangle
Deep fascia of the pelvic floor
Deep perineal pouch
Perineal membrane (pierced by vagina and urethra)
Superficial perineal pouch
Perineal fascia
(Deep layer: Scarpa’s fascia, superficial layer: Camper’s fascia)
Identify the main muscles forming the pelvic floor and state their nerve supply.
Outline the potential consequences of damage to this area.
Pelvic floor muscles:
- Levator Ani: Pubococcygeus, puborectalis and iliococcygeus
Innervated by the pudendal nerve (S2-S4)
- Coccygeus (aka ischiococcygeus)
Innervated by the anterior rami of S4 and S5
Functions: Support organs, maintain continence and resist intrabado./pelvic pressure
Damage to the area may lead to prolapse and incontinence.
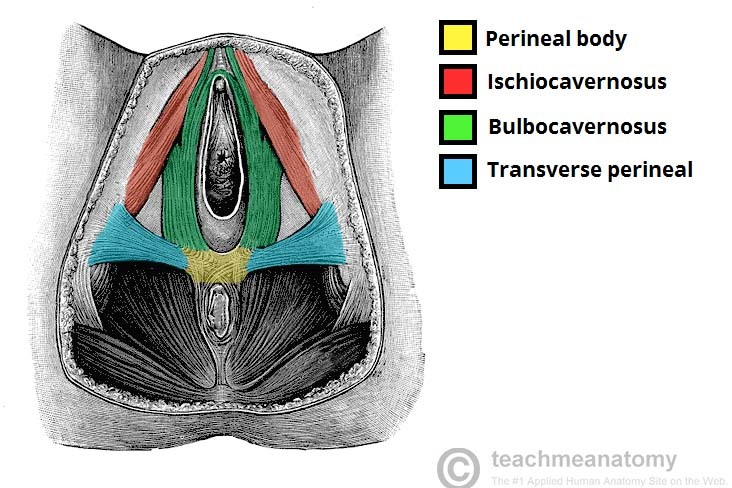
Explain the significance of the perineal body and outline the potential consequences of damage to this structure
*Clinical link
The perineal body is a thickening of fibromuscular tissue.
Located between the vagina/bulb of the penis and the anus.
Functions: An attachment site for muscles of the pelvic floor/perineum and the perineal membrane. Supports against prolapse in females
- Attaching muscles = BLP (Levator Ani, bulbospongiosus and Superficial and deep tranverse perineal)
Consequences of damage: Increased risk of prolapse, incontinence
- Episiotomy: A ‘managed’ incision made to the perineum during childbirth to prevent the perineal body and anal sphincter from tearing.
Identify the organs of the pelvis
Urinary: Pelvic uteter, urinary bladder, urethra
Genital:
- Male: Ductus deferens (vessel for sperm transport), seminal vesciles, prostate
- Female: Uterine tubes, ovaries, uterus, vagina
Digestive: Rectum, anal canal
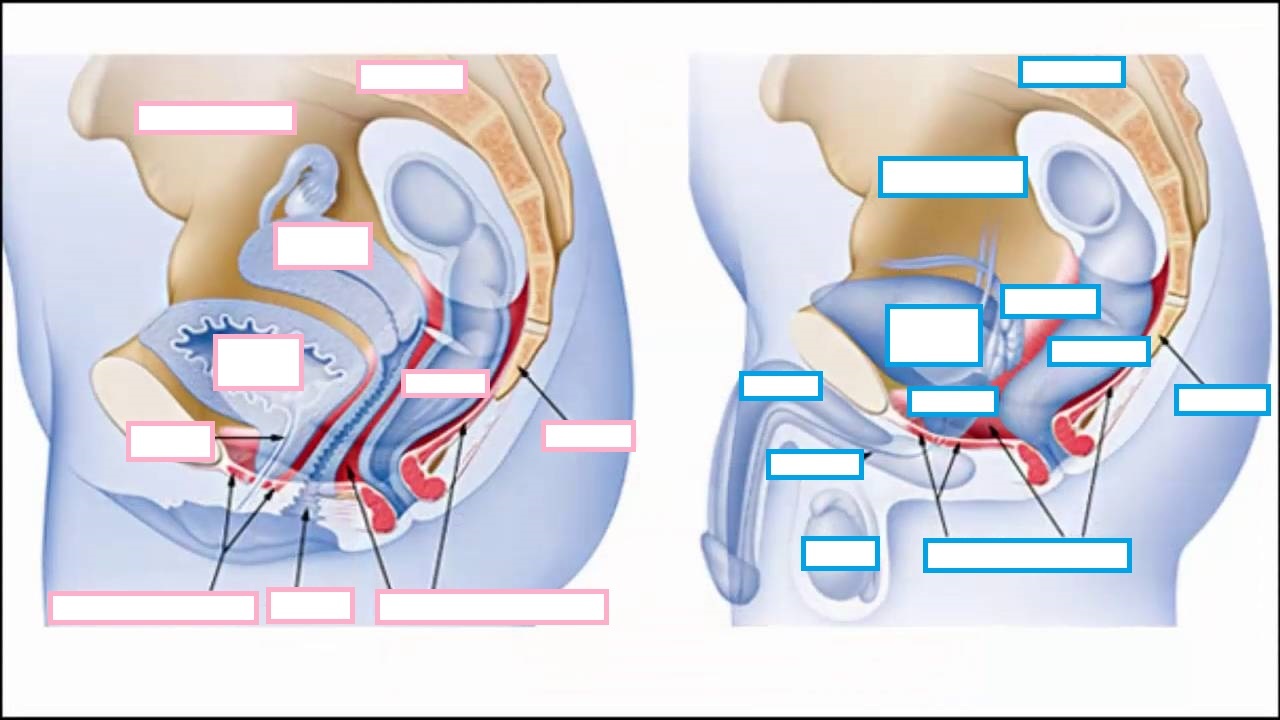
Describe the recesses formed by the peritoneum and state their significance
Double foldings of peritoneum drape over the pelvic organs forming the:
Females:
- Rectouterine pouch of Douglas: Between the uterus and the rectum. This is the most inferior point in the female body. Fluid may collect in this recess when standing or supine.
Radiopaedia: Abscess, infection, ascites, haemoperitoneum, and even intraperitoneal drop metastases preferentially collects here.
- Vesicouterine pouch: Between the uterus and the bladder.
Males:
- Rectovesical pouch: Between the bladder and the rectum

Identify the main branches of the internal iliac artery.
(ILGPIMVOU)
Describe their location and basic distribution.
Common iliac artery ➙ External and internal iliac branches
Internal iliac artery ➙ Anterior and posterior divisions
Divides at the superior border of the greater sciatic foramen
Branches of posterior (first 3) and anterior divisions:
Iliolumbar
Lateral sacral
Gluteal (superior and inferior)
Pudenal (internal)
Inferior vesicle (vaginal in females)
Middle rectal
Vaginal
Obturator
Umbilical and uterine (females only)
- The umbilical artery (carries deoxygenated blood to the placenta) obliterates to become the medial umbilical ligament
List structures that may be palpated by rectal examination
Females: Anus, uterus
Males: Anus, prostate
List structures that can be palpated by vaginal examination
Visual inspection ➙ speculum ➙ palpation
PV exam: Vagina, cervix, fornices
Bimanual exam: Uterus, ovaries and uterine tubes
Describe the course of the nerve supplies to the pelvic and urogenital diaphragms and perineum
The pudendal nerve (S2-S4)
- Motor to pelvic floor muscles and sensory to the perineum
- Exits the pelvis via the greater sciatic foramen
- Re-enters the pelvis via the lesser sciatic foramen
- Travels laterally along the ischioanal fossa (via the pudendal/Alcock’s canal)
- Divides into serveral branches
Ischioanal fossae: Explain borders, content, normal function and how infection can spread around the region
Borders: Located laterally to the anus within the anal triangle
- See image
Content: Adipose tissue, pudendal/Alcock’s canal (contains pudendal nerve and internal pudendal artery/vein), inferior rectal nerve and vessels, lymphatics
Normal function: Allow for the expansion of the anal canal during defecation, supports the anal canal
Spread of infection: Vulnerable to spread of infection from the anal canal. Abscesses may form and infection may spread to the opposite fossa, passing behind the anal canal. Fistulas may form (with the anus)

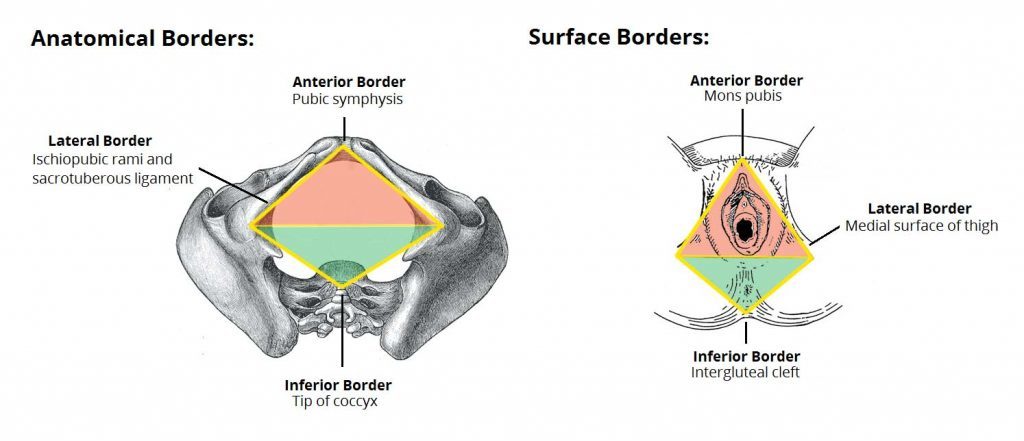
Outline the borders of the perineum and its divisions
Anterior: Pubic symphysis
Lateral: Ischiopubic rami and sacrotuberous ligament
Posterior: Tip of the coccyx
Divided into the anal and urogential triangles via a ‘line’ between the ischial tuberosities
Axillary nodes may be removed in patients with breast cancer. This procedure may lead to damage to which nerve?
Long thoracic nerve
Innervates the serratus anterior muscle.
Damage causes winging of the scapula.
Thoracodorsal nerve may also be injured
Innervates latissimus dorsi
Name the layers of the abdominal wall

Outline the contents of the deep perineal pouch of the urogenital triangle
A potential space between the deep fascia of the pelvic floor muscles and the perineal membrane
Females:
- Urethra
- External urethral sphincter
- Vaginal
Males:
- Bulbourethral/Cowper’s glands (watery pre-ejaculate)
- Deep transverse perineal muscles

Outline the borders of the perineum and name the structure which allows for division into anterior and posterior triangles
Anterior: Pubic symphysis
Lateral: Ischiopubic rami and sacrotuberous ligament
Posterior: Tip of the coccyx
The ischial tuberosities mark the division of the perineum
***Perineal membrane (layer of strong fascia) only seen in the urogenital triangle, not the anal triangle***























-
STIs (7.1)21
-
Module Workshops69
-
Gametogenesis (7.2)8
-
DUB, Ovarian Function and Anovulation (7.2)23
-
Cancers of the female reproductive tract and breast structure (7.1)16
-
Infertility (7.2)13
-
PBL Learning Objectives74
-
Pharmacology24
-
Puberty (7.2)10
-
Pre-natal nutrition, placenta and foetal membranes (7.3)8
-
Physiology and Pathophysiology of Pregnancy 7.325
-
Menarche, menopause and beyond (7.2)13
-
Conception and fertility (7.3)4
-
Anatomy of the male urogenital tract (7.4)7
-
Prostate pathology: BPH, prostitis and prostate cancer (7.4)11
-
Male Sexual Function and Dysfunction (7.4)5
-
Renal physiology: Function, structure and ultrafiltration (7.5)12
-
Assessment of kidney function and disease (7.5)14
-
Kidney pathology (7.5)28
-
Urinary Tract Infection (UTI) (7.5)14
-
Potassium Homeostasis (7.6)6
-
Renal Acid-Base Regulation (7.6)10
-
Menstrual Cycle (7.1)6
-
Nephrotic and Nephritic syndromes (7.7)9
-
Reabsorption (salt, water and glucose) and Osmoregulation (7.6)12
-
Diuretics: Complications and actions (7.6)6
-
Proteinuria (7.6)8
-
Chronic Renal Failure Pathophysiology (7.7)5
-
Disorders of ECV (7.6)4
