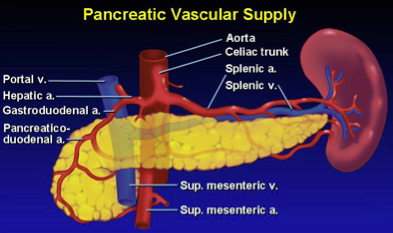
which arteries supply the pancreas?
celiac and SMA
exocrine pancreas is ___% pancreatic mass
exocrine pancreas makes ______
85%
digestive enzymes, water, bicarb –> duodenum
pancreatic embryology
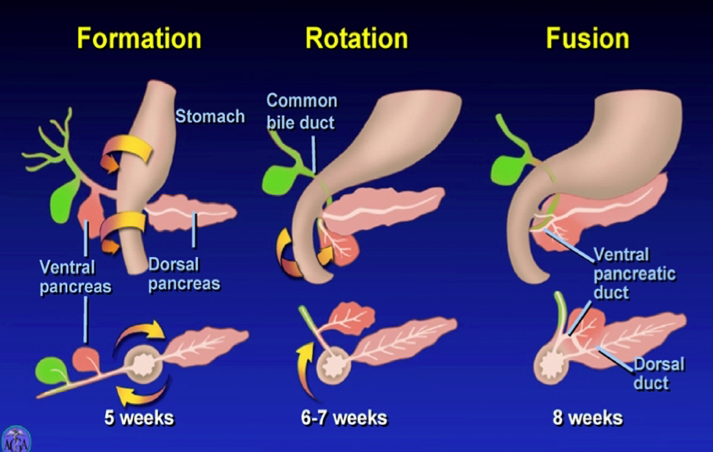
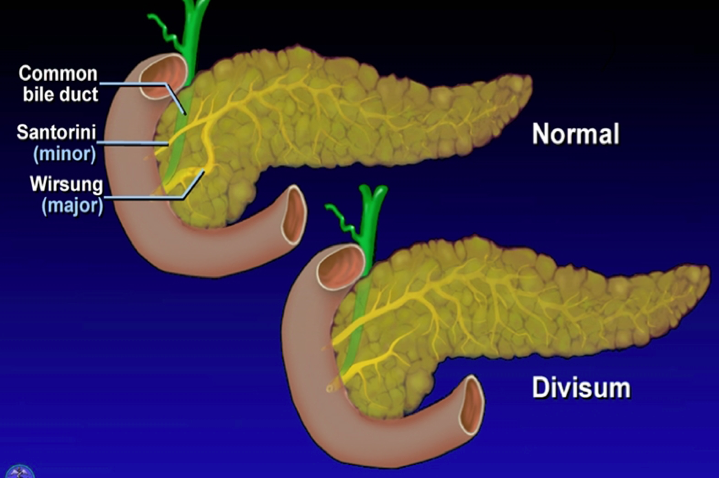
common variations in pancreatic duct anatomy
90%- Santorini and major duct connected
10% - fusion does no occur = pancreas divisium –> higher risk for pancreatitis
regulation of pancreas secretion
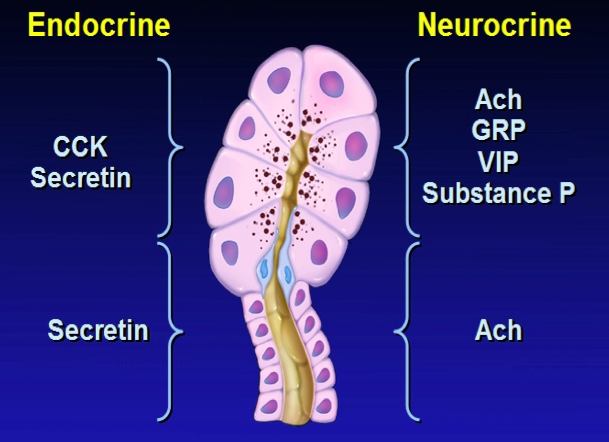
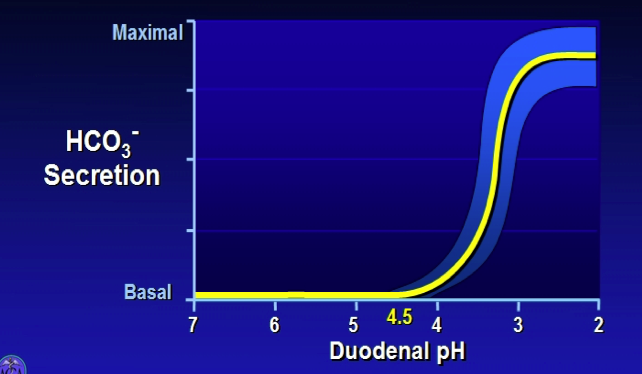
what determines bicarb secretion from the pancreas?
duodenal pH >4.5 - sensed in s/secretin cells
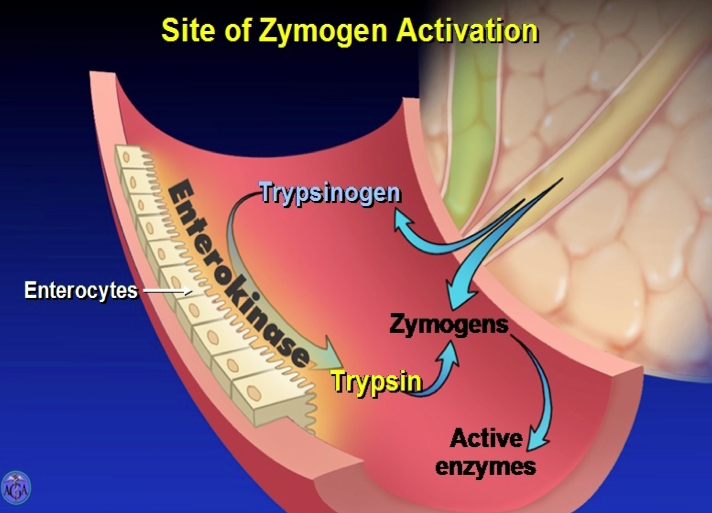
how does the pancreas avoid digesting itself?
pancreatic enzymes are stored in pancreas and secreted into duodenum as PROENZYMES. Enterokinase at brush border in duodenum converts trypsinogen –> trypsin. Trypsin makes the other zymogens –> active enzymes.
amylase and lipase are stored in active forms b/c there is no starch or TG in the pancreas to be digested
5 protective mechanisms in the pancreas
- synthesis of enzymes as inactive zymogens
- trypsin inhibitor packaged in zymogen granules
- segregation of enzymes in membrane bound compartments
- enterokinase restricted to small intestine
- acidic pH w/in zymogen inactivates Trypsin
Labs in acute pancreatitis
WBC: often elevated
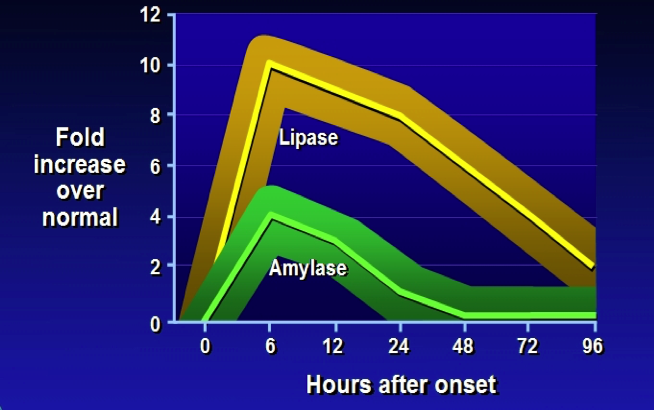
Amylase: leaks from inflamed pancreas. high sensitivity, low specificity
Lipase: sensitive as amylase, but more specific , and remainvs elevated
Atlanta criteria for Acute pancreatitis
two or more of the following:
- abdominal pain consistent w/ acute pancreatitis: sudden onset upper abdominal pain, often radiating to upper back. steady pain w/ “boring” quality.
- elevated amylase or lipase >3x normal
- confirmatory finding on CT
normal amylase, high lipase - interpretation?
delayed presentation of acute pancreatitis
how do gallstones cause pancreatitis?
migrate to the cystic duct –> common duct –> can obstruct the ampulla of vater –> pancreatitis and/or cholangitis

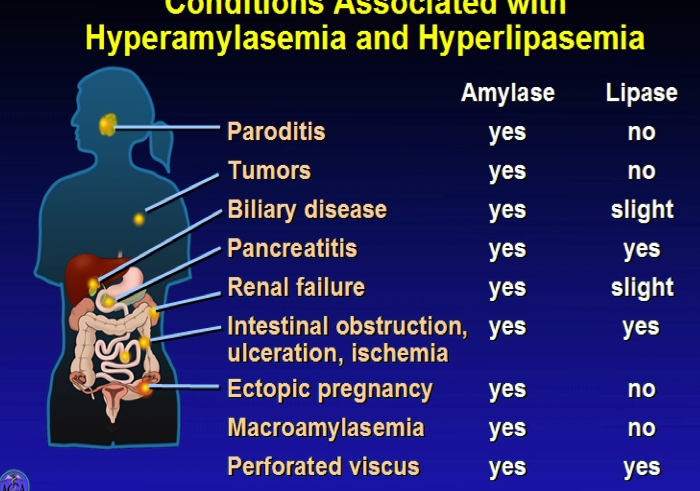
which pancreatic hormone is most specific in dx pancreatitis?
lipase
lots of things can cause elevation of amylase
How do you assess the severity of pancreatitis?
Bedside eval
BISAP >2
- BUN>25, impaired mental status, SIRS, Age>60, pleural effusions
BUN >22
CRP >125 @48 hrs
SIRS persisting through 48 hours
what is SIRS?
presence of at least 2
- pulse >90 BPM
- RR >20 or PCO2<32mm Hg
- T> 100.4 or <96.8
- WBC> 12K or <4K
what are these and prognosis for each
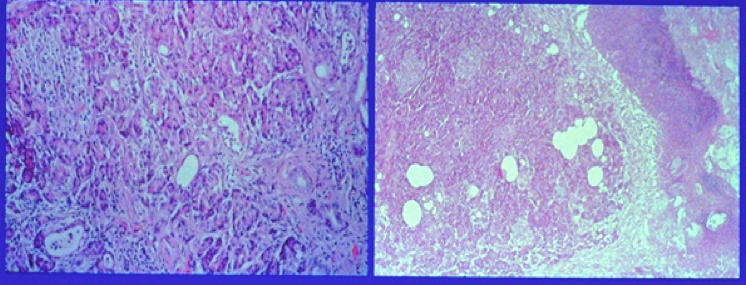
left = interstitial
- very low mortality and infection (<1%)
right = necrotizing
- high infection rate (30-50%)
- mortality 10-30%
what causes acute pancreatitis?
- alcohol
- gallstones
- idiopathic
- other: high TGs, autoimmune, drugs, IBD, infectious, neoplasm, toxic, iatrogenic (ERCP), trauma, scorpion
inherited causes of pancreatitis
altered enzyme activity: trypsinogen mutations
abnormal ion movement: CFTR mutation
metabolic: familial hypertriglyceridemia (TGs <1000)
tx for acute pancreatitis
nothing to tx underlying pathophys
supportive care: IV fluids/lytes (EARLY and w/ Lactate Ringers), montioring, analgesia + antiemetics
other txs: Abx, NG tube, nutritional support, urgent ERCP (if gallstones)
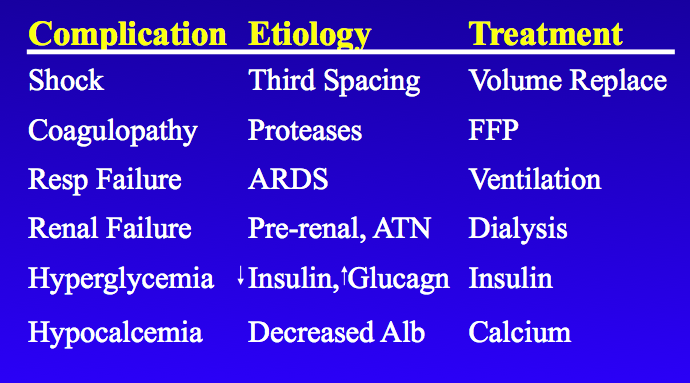
systemic complications of acute pancreatitis
local complications of acute pancreatitis
fluid collection
necrosis
infection
ascites
erosion into adjacent structures
GI obstruction
hemorrhage
what is a pancreatic pseudocyst?
localized collection of pancreatic fluid that develops >4 wks after pancreatitis onset
how to distinguish from true pancreatic cysts: absence of epithelial lining
how to prevent infection in acute pancreatitis pt?
enteral feeding through jejunal tube! - to maintain gut barrier function
*abx use is controversial for prophylaxis
causes of death in acute pancreatitis
early <1 wk: SIRS, multiorgan failure
late: multiorgan failure, pancreatic infections/sepsis






-
Toxicology Pharm25
-
Gastric Secretions / Peptic Ulcer Disease25
-
Liver Structure and Function24
-
GI Pharm35
-
Metabolic/ Storage Diseases of Liver35
-
Alcoholic Liver Disease12
-
Non-alcoholic Fatty Liver Disease5
-
Pediatric GI30
-
Pathogenesis of Cirrhosis/Liver Tumors22
-
Viral Hepatitis29
-
Disorders of Gallbladder and Biliary Tract42
-
Pancreas Function/Disorders42
-
Pancreatic Carcinoma13
-
Benign Anorectal Disease21
-
IBD25
-
Maldigestion and Malabsorption30
-
Esophageal Physiology, Motility, GERD6
-
Pathology of Mouth and Esophagus16
-
Pathology of Gastric Diseases11
-
Appendicitis and Diverticular Disease3
-
Imaging GI tract3
-
Enteric Nervous System9
-
Approach to Diarrhea8
-
IBD Tx5
-
Large Bowel Neoplasm10
-
Autoimmunity and the Liver6
