List three reasons why rx not accurate for cardiac evaluation
1) Variations in normal
2) Effect of positioning on appearance
3) Poor correlation between morphological and physiological abnormalities
Which radiographic projections comparatively influence the appearance of the cardiac silhouette most profoundly? How / why?
DV vs VD
DV: Diaphragm billows forward, displacing heart cranially and to the left to a varying degree -> more pronounced in medium / large breeds
VD: Magnification of the heart in LARGE BREEDS due to distance from plate
Describe the vertebral heart scoring system. Why is it used?
- Theoretically allows normlisation for body size
Technique:
- Measure long axis and short axis -> SUM
- Measure from cranial margin of T4
Normal: 8.7-10.7 (Too variable!)
**Up to 1.0 may vary with cardiac / resp cycle**
=> Best used for serial images in same patient
DOES NOT PERFORM BETTER THAN QUALITATIVE
What is the most common chamber dilation in the dog? Why?
LA -> Prevalence of MMVD
Why does LA dilation result from L->R shunting?
Pulmonary overcirculation and VOLUME OVERLOAD
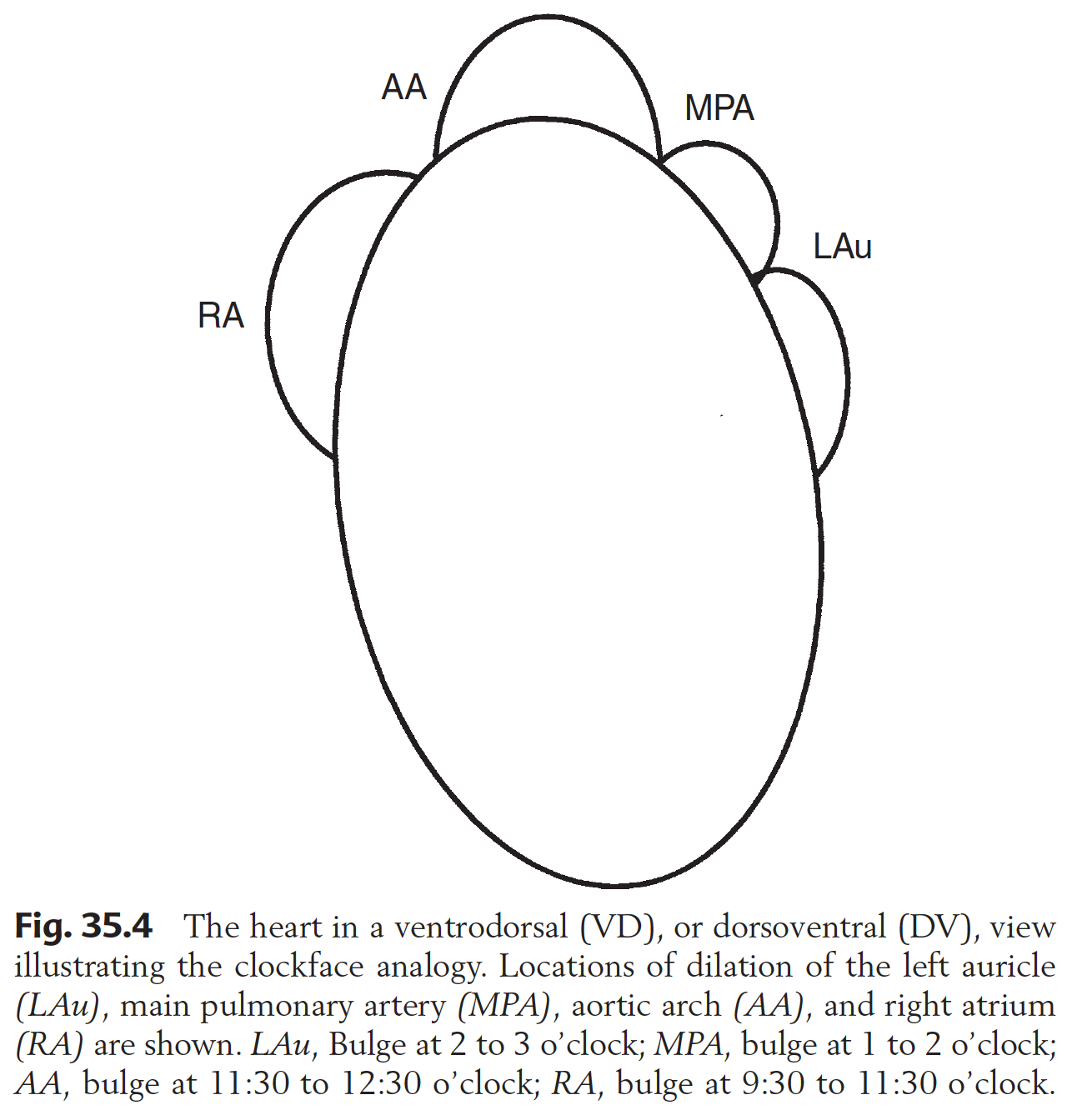
In the DV projection, what structures are identified at the 12-1; 1-2; and 2-3 positions on the clock face? Where is the RA identified?
Why do dogs with LAE cough?
Possibly some inpingment from LA BUT USUALLY DUE TO CHONDROMALACIA
-> NO association between canine CHF and coughing
How can LAE and TB LN+ be distinguished?
BOTH cause divergence of prinipal bronchi
LAE: Ventral to bifurcation
TB LN: Dorsal to bifurcation (typically)
List radiographic features of LAE in the dog
Lateral:
Dorsocaudal bulge
Flattening / concavity of caudal margin
Loss of cardiac waste
DV:
Divergence of principal bronchi
“Double wall” - appearance of enlarged LA superimposed on heart
L Auricular enlargement / displacement
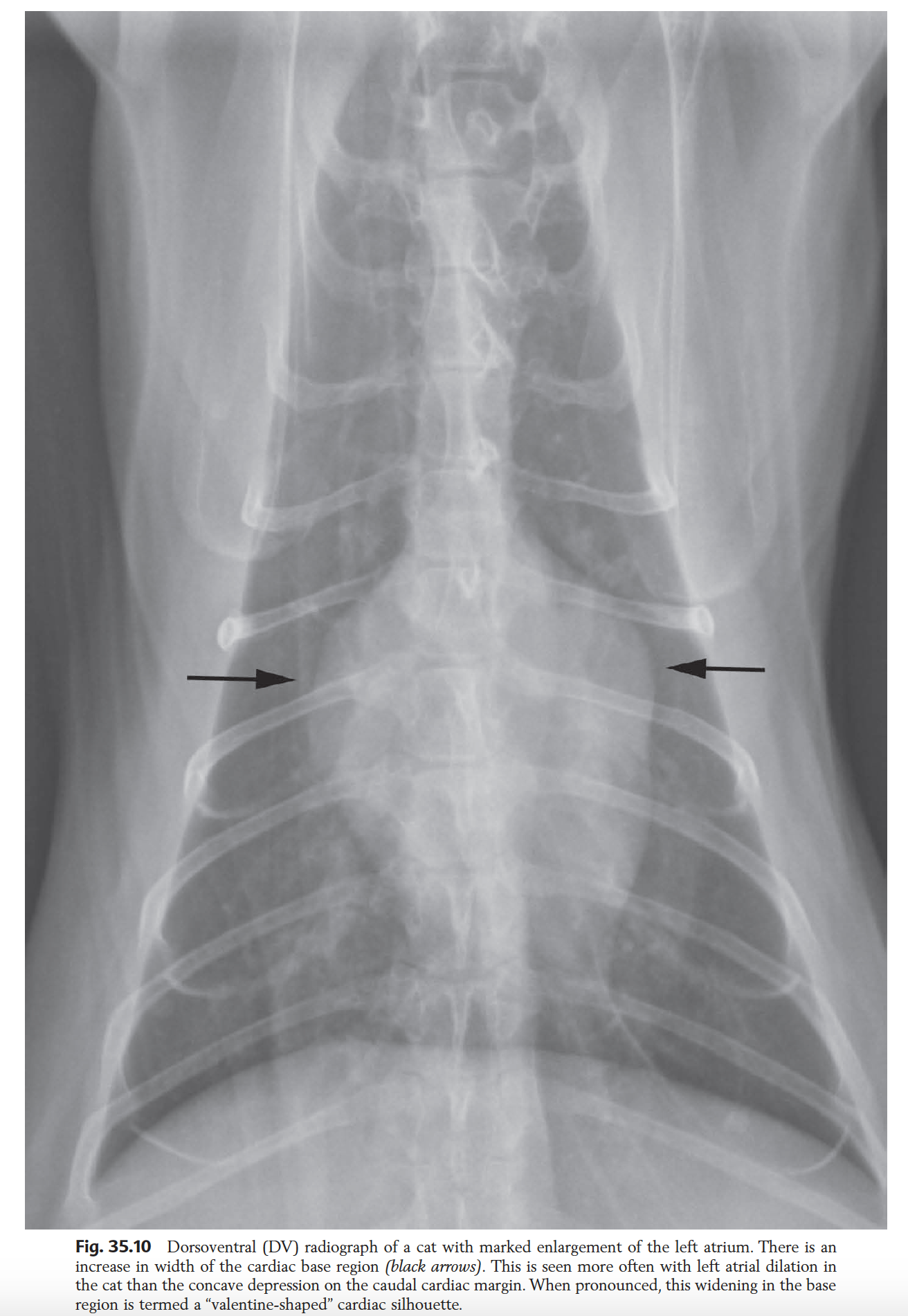
List radiographic features of LAE in the cat
**MAY APPEAR NORMAL**
Lateral:
- Concavity of caudal margin
DV:
- Valentine shape heart -> Due to increased diameter of heart base. DOES NOT REFLECT BIATRIAL DILATION!!!!
List features of LV enlargement (dog and cat same)
Lat:
- Elongation -> Secondary elevation of trachea
=> Narrowing of angle between trachea and thoracic vertebrae
VD/DV:
- Rounding of left heart border
- Blunted apex
Provide examples that cause LV eccentric vs concentric hypertrophy
Eccentric => INC PRELOAD
- PDA
- MVD
Concentric => INC AFTERLOAD
- Ao Stenosis
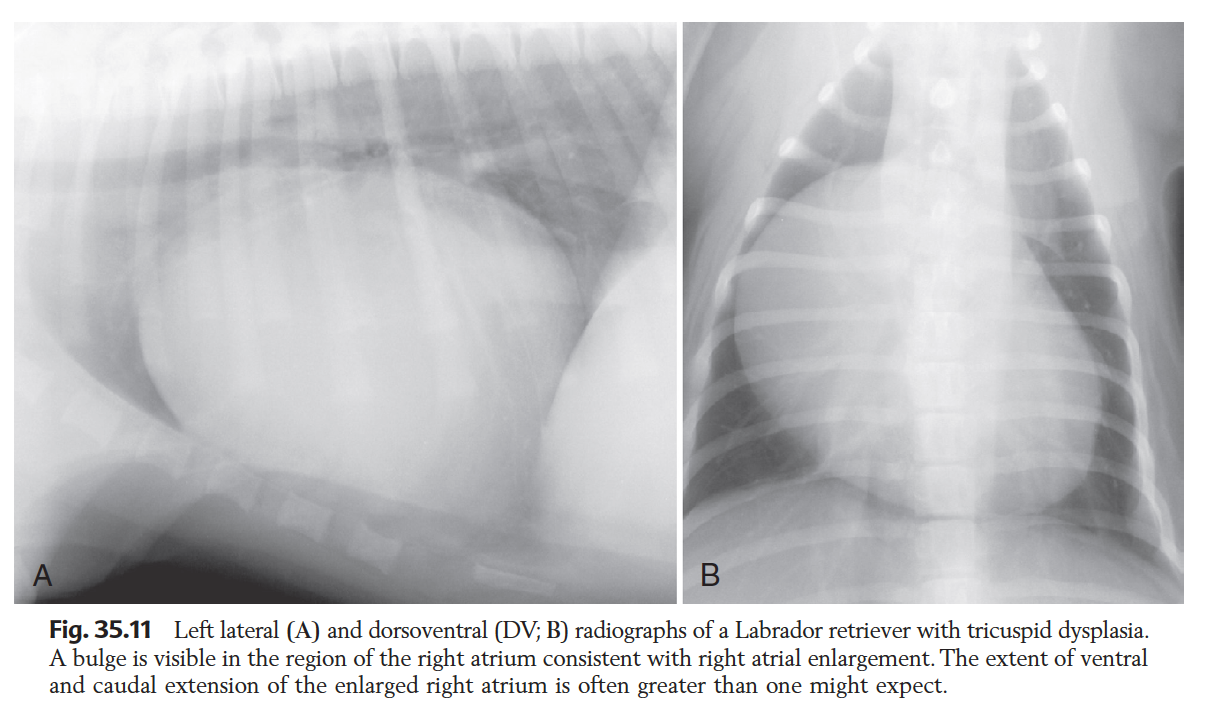
Cause of isolated RA enlargement?
RARE
Tricuspid dysplasia
Rx features of RAE
Lateral:
- Enlargement at craniodorsal aspect -> NOTE may reflect enlargement of aorta or MPA
DV/VD
- 9-11 o clock bulge
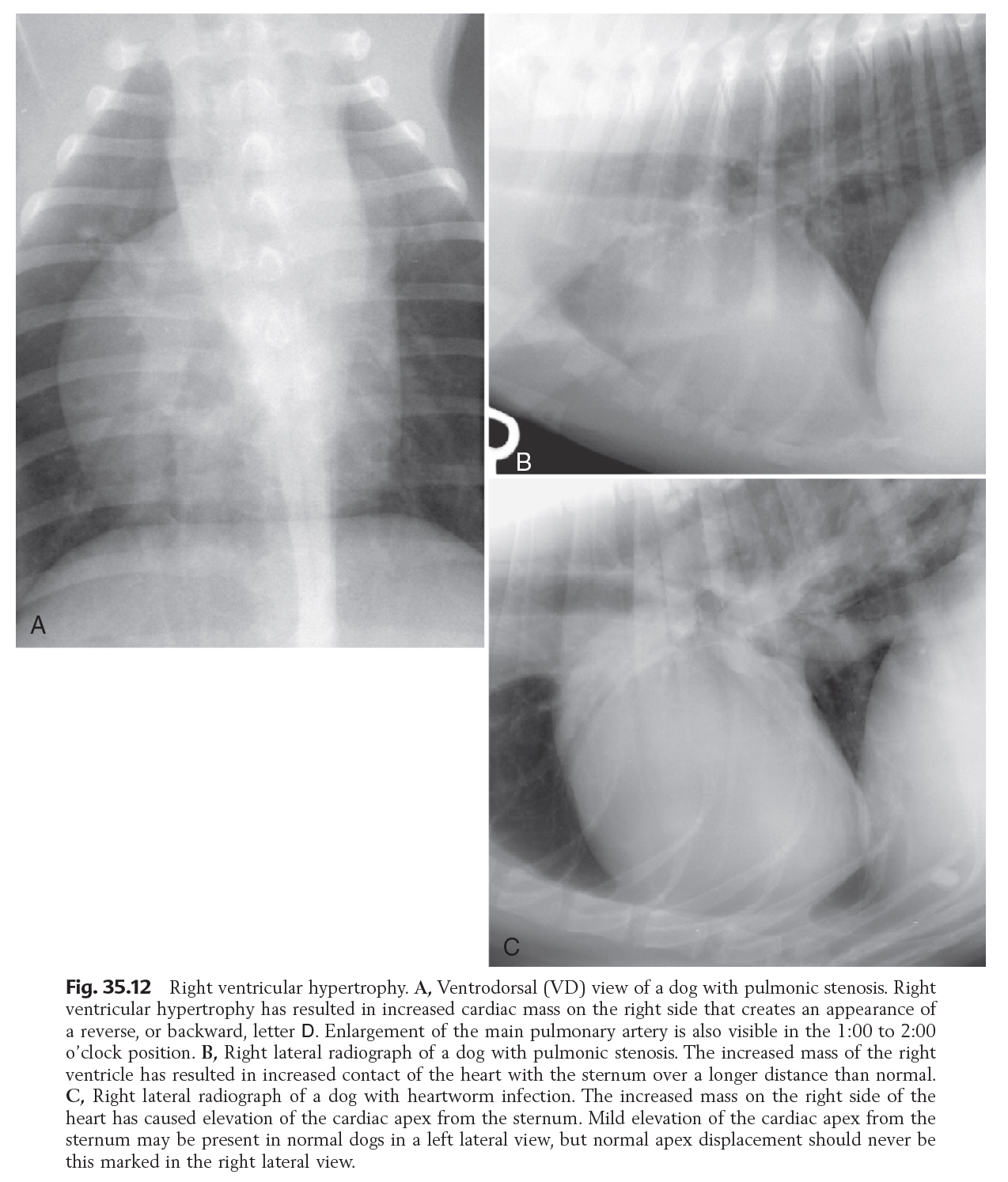
Hypertrophy of which chamber may be identifiable radiographically?
RV -> More so than LV
Possibly due to thinner wall -> more obvious changes
Define the amount of sternal contact described in normal dogs of different breeds
Deep chested (Dobi, wolfhound): 1.5-2 ICS
Average dog: 2.5-3 ICS
Barrel chested (bulldog): 3-3.5 ICS
>3 often described to support RV enlargement
Rx features of RV Enlargement
Lat:
- Increased sternal contact (Approx > 3 ICS)
- Elevation of heart apex from sternum
DV/VD
- Reverse D
What 2 measures are used to determine CaVC enlargement?
- diameter > length of 5th or 6th thoracic vertebral body
- diameter > 1.5x descending Ao
=> NOTE: Variability with cardiac and resp cycle. Should be consistent finding
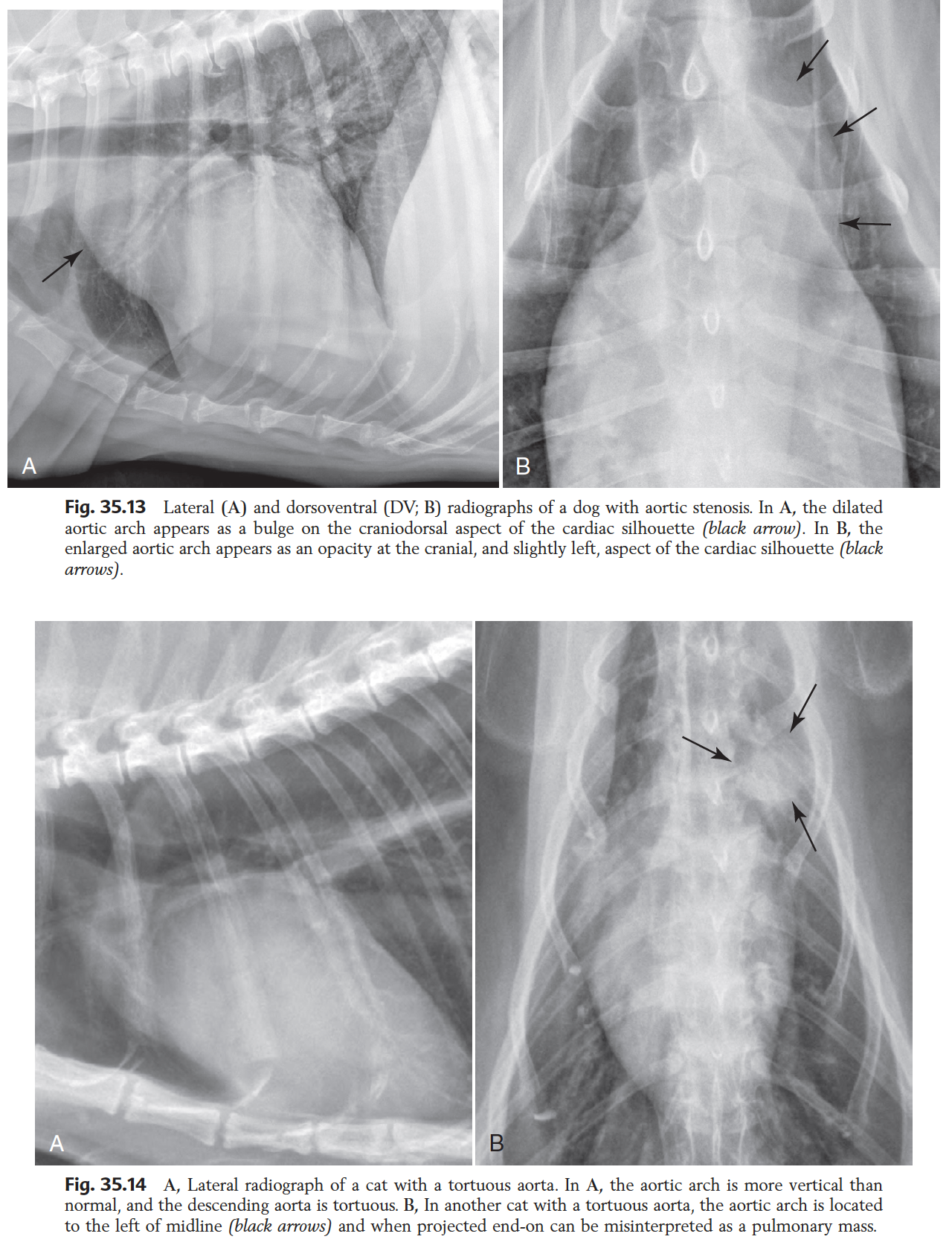
Rx features of Ao enlargement
Lat:
- Inc. mass at craniodorsal aspect
VD/DV:
- Widening of precardiac mediastinum
- Focal bulge (e.g. Ao stenosis, PDA)
- **BEWARE** older cats with tortuous Ao, may be projected laterally to left, and appear as pulmonary nodule
Causes of RV hypertrophy
INC AFTERLOAD:
- Pulm stenosis
- Pulm hypertension (e.g. heartworm)
Which projection is best used to evaluate the size of the cranial pulmonary arteries and veins?
LEFT LATERAL
=> in right lateral, often superimposed vessels interfere
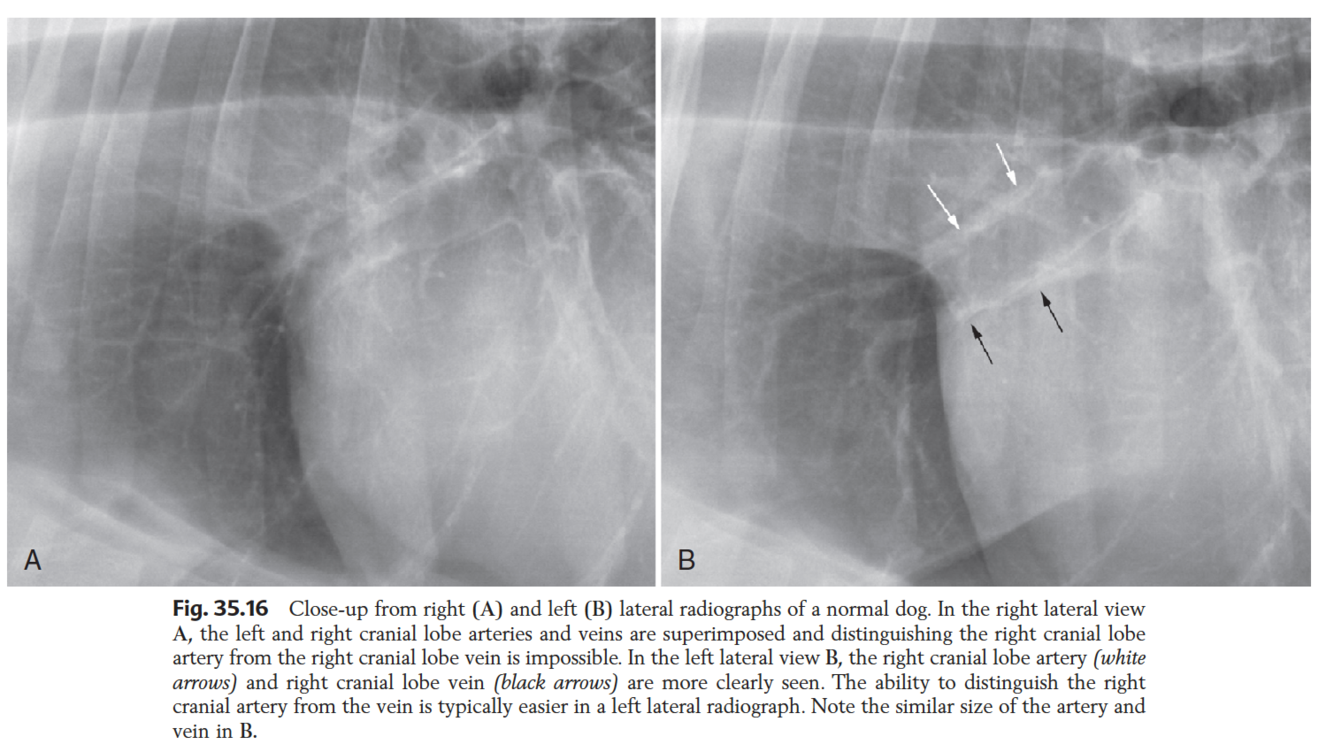
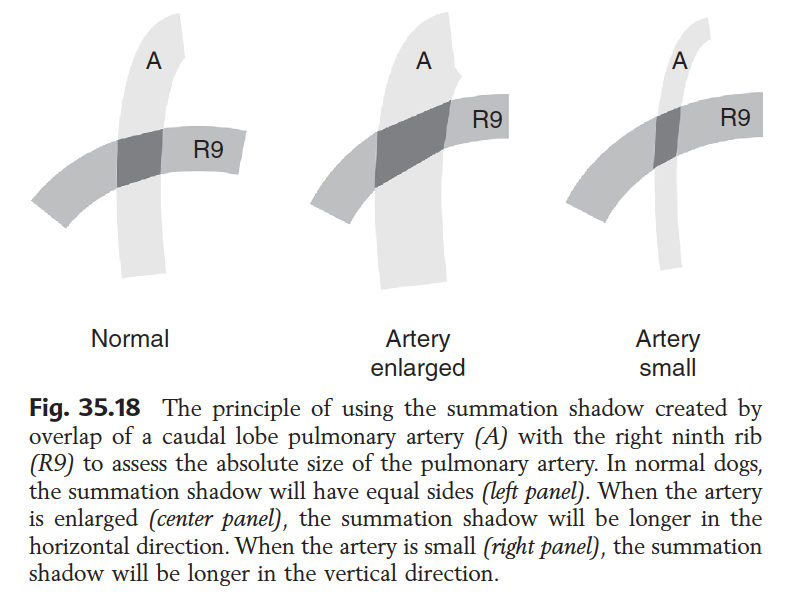
Which measures are used to evaluate peripheral pulm art and vvs?
- Are they similar in size?
- Relative to thickness of 9th rib
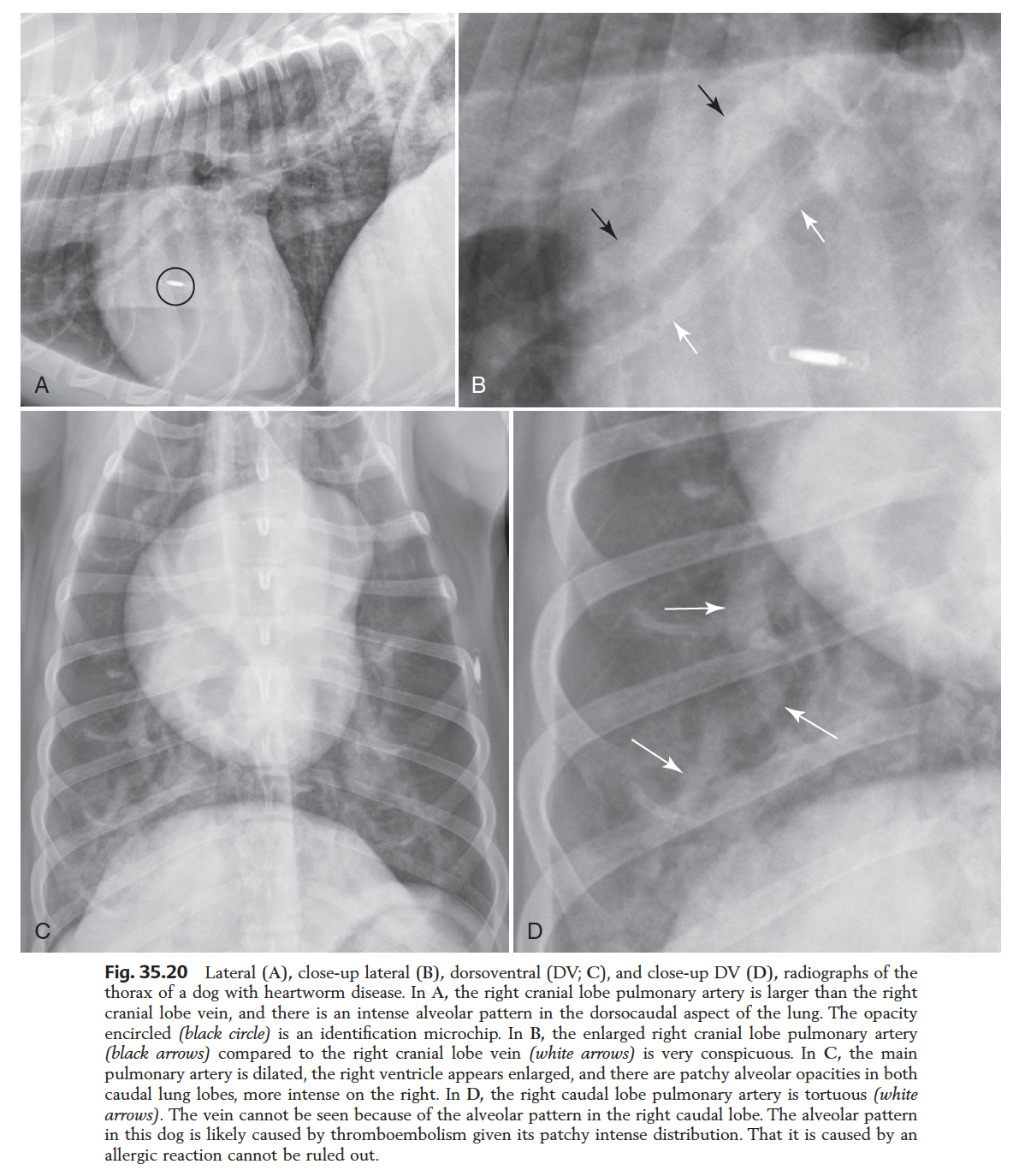
BOX: Enlarged pulm a and v
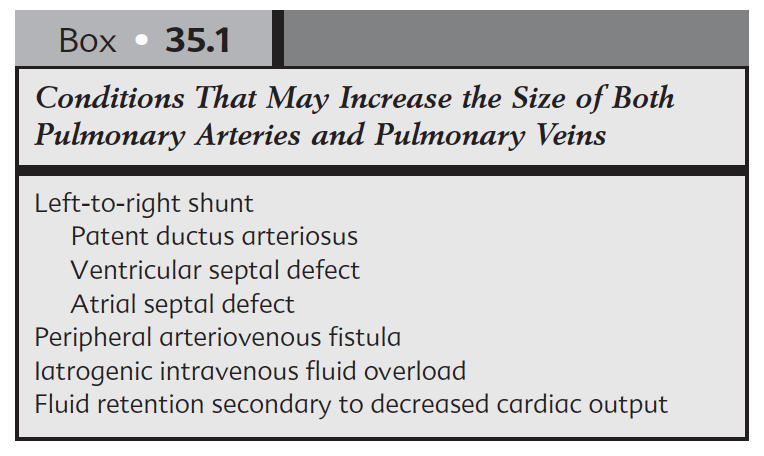
What is the most common cause of pulm art distension without vein?
Pulmonary hypertension 2ry to HEARTWORM
































-
1. Radiation Protection and Physics of Diagnostic Radiology36
-
2. Digital Radiographic Imaging23
-
3. Dental technique8
-
4. Physics of Ultrasound30
-
5. Principles of CT and MRI33
-
6. Contrast media34
-
7. Intro to radiographic interpretation2
-
8. Radiographic anatomy of axial skeleton10
-
9 - Principles of Interpretation of Axial skeleton16
-
10 - Canine and Feline dental disease65
-
11. Nasal cavity37
-
12. MRI Brain47
-
14. XR Vertebrae41
-
15. CT / MR Spine69
-
16. Radiographic anatomy of appendicular skeleton28
-
17. Principles Appendicular skeleton5
-
18. Orthopaedic Diseases of Young and Growing Dogs and Cats51
-
19. Fracture Healing and Complications in Dogs48
-
20. Bone tumours and infections21
-
21. Joint Disease68
-
28. Principles of interpretation - Thorax6
-
29. Larynx and trachea38
-
30. Oesophagus64
-
31. Thoracic wall12
-
33. Mediastinum35
-
32. Diaphragm38
-
34. Pleural Space17
-
35. Cardiovascular system (+ extra bits)72
-
36. Lung31
-
38. Principles of interpretation - Abdomen2
-
Chapter 39 - Peritoneal Space52
-
40 - Liver and Spleen43
-
41 - Kidneys and Ureters40
-
42 - Urinary Bladder31
-
43 / 44 - Urethra / Prostate30
-
45 - Uterus, Ovaries and Testes30
-
46 - Stomach35
-
47 - Small intestine49
-
48 - Large Bowel22
-
THE MOST IMPORTANT QUESTIONS!328
