List 3 key features of headless compression screw
- Differential thread pitch –> interfragmentary compression
- Headless design allows implantation beneath bone surface
- Cannulated to allow for precise insertion using guide wire
- Self-drilling/self-tapping,
- Comprehensive portfolio: 2.0, 2.5, 3.0, 3.5, 4.0, 4.5, 5.5, 6.5, 7.5 mm
- Titanium alloy (Ti-6Al-4V ELI)
- Short and long thread lengths for treating a wide range of anatomical regions
- Sterile and non-sterile packaging options
- Color-coded instrumentation
- Modular sets for flexibility
List the 4 forces to be considered in fracture repair
- Compression
- Tension
- Bending
- Rotation
List 4 principles of biological osteosynthesis
- Indirect fracture reduction using limited surgical approaches
- Stabilisation using bridgingimplant rather than anatomic reconstruction and rigid fixation
- Limited reliance on internal secondary implants (cerclage, lag etc)
- Limited (if any) use of bone grafts
List primary and secondary fracture fixation implants
Primary:
- Plate
- IM pin
- ILN
- ESF
Secondary:
- Cerclage
- K-wires
- Lag screws
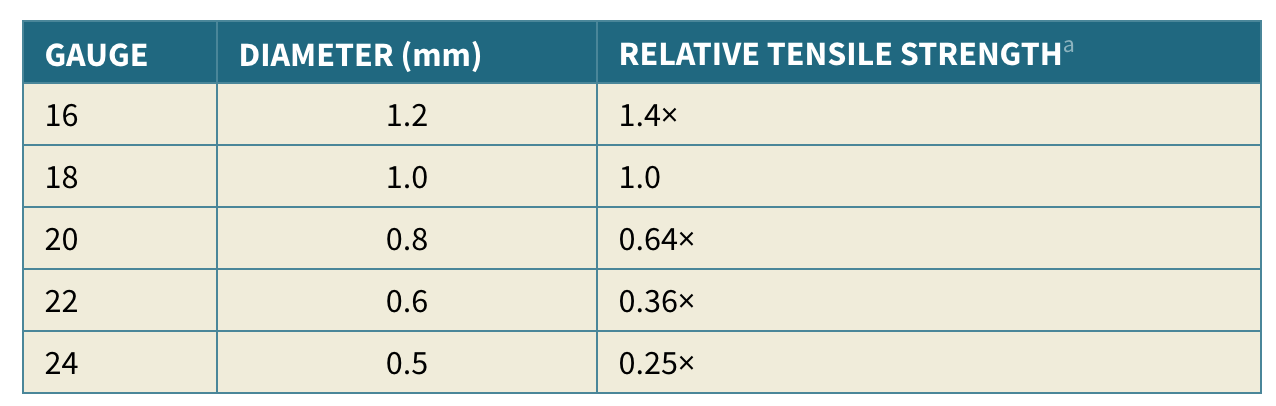
What is the formula for tensile strength of a wire?
πr2
Relative to the tensile strenght of a 1.0mm wire, what is the strength of a 0.8mm wire?
And 1.2?
- 8mm –> 0.64 x strength of 1.0mm wire
- 2mm –> 1.4 x strength of 1.0mm wire
Name two techniques for securing cerclage wire oblique to bone axis
Skewer pin or notch in cortex
What is purpose of hemi-cerclage?
Improved alignment (only resists bending in one plane)
How many twists must be left on cerclage wire afetr twist knot?
1 to maintain tension but advise 3
Name 4 cerclage wire ‘configurations’
- Twist
- Single loop
- Double loop
- Cable + crimp cerclage
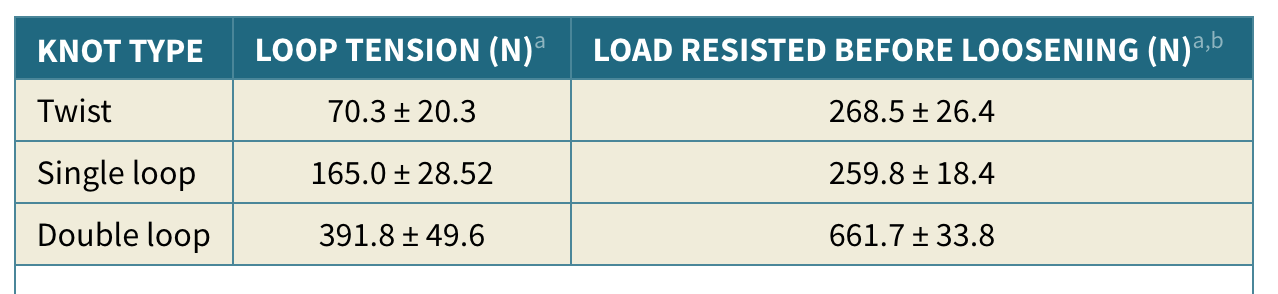
How does load resistance differ between twist, single loop vs double loop cerclage wire?
- Similar load resisted between twist vs single loop (approx 260N), althoguh single loop achieved higher initial tension (165N vs 70N).
- Double loop –> higher initial tension (390N) and higher load resisted (660N)
What % reduction in resting load was noted when cerclage wire twist was bent over?
45-90%
i.e. they recommend keep straight and cut short rather than bending
What % reduction on bone diameter –> resting tension of cerclage wire <30N?
1%!
i.e. if fragments move at all, cerclage becomes ineffective
What is recommended fracture legth:bone diameter ration for application of cerclage wire?
Fracture x 2.5-3 lenght of bone diameter
What is recommended distance between cerclage wires?
Half bone diameter
Above what diameter are k-wires called steinmann pins
1.6mm
How does area moment of inertia relate to radius of a cylinder?
r4
N.B. Uses r4, doesnt equal r4
What is area moment of inertia of 1.1mm pin vs 2.0 mm pin?
- 1 mm = 0.07 mm4
- 0 mm = 0.8 mm4

When IM pin is only intramedullary device, what is recommeded size?
>70% medullary diameter
What is more stable rush pins (dynamic crossed pins) or conventional cross pins?
Conventional
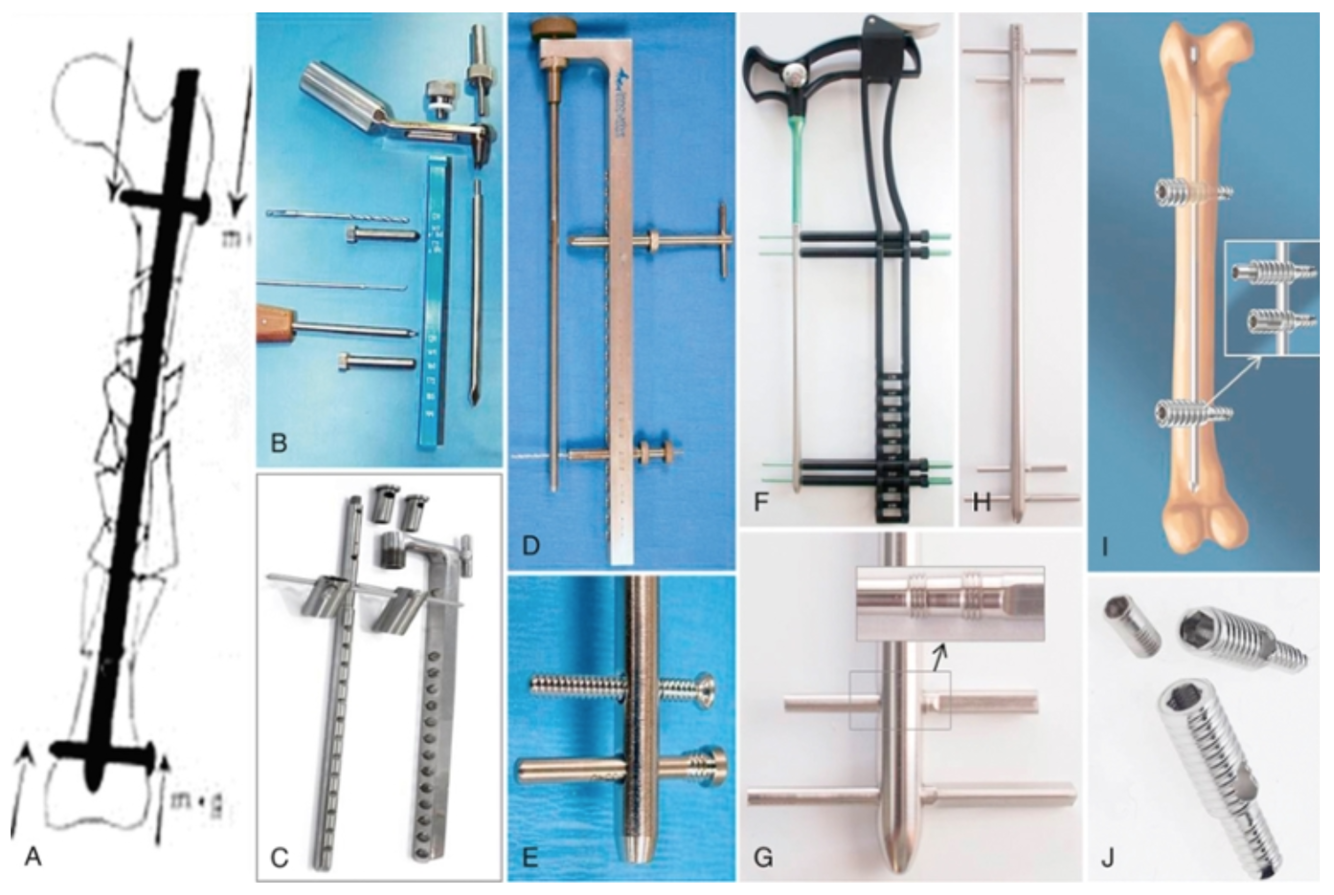
Nme the ILN types:
D + E
F + G
I + J
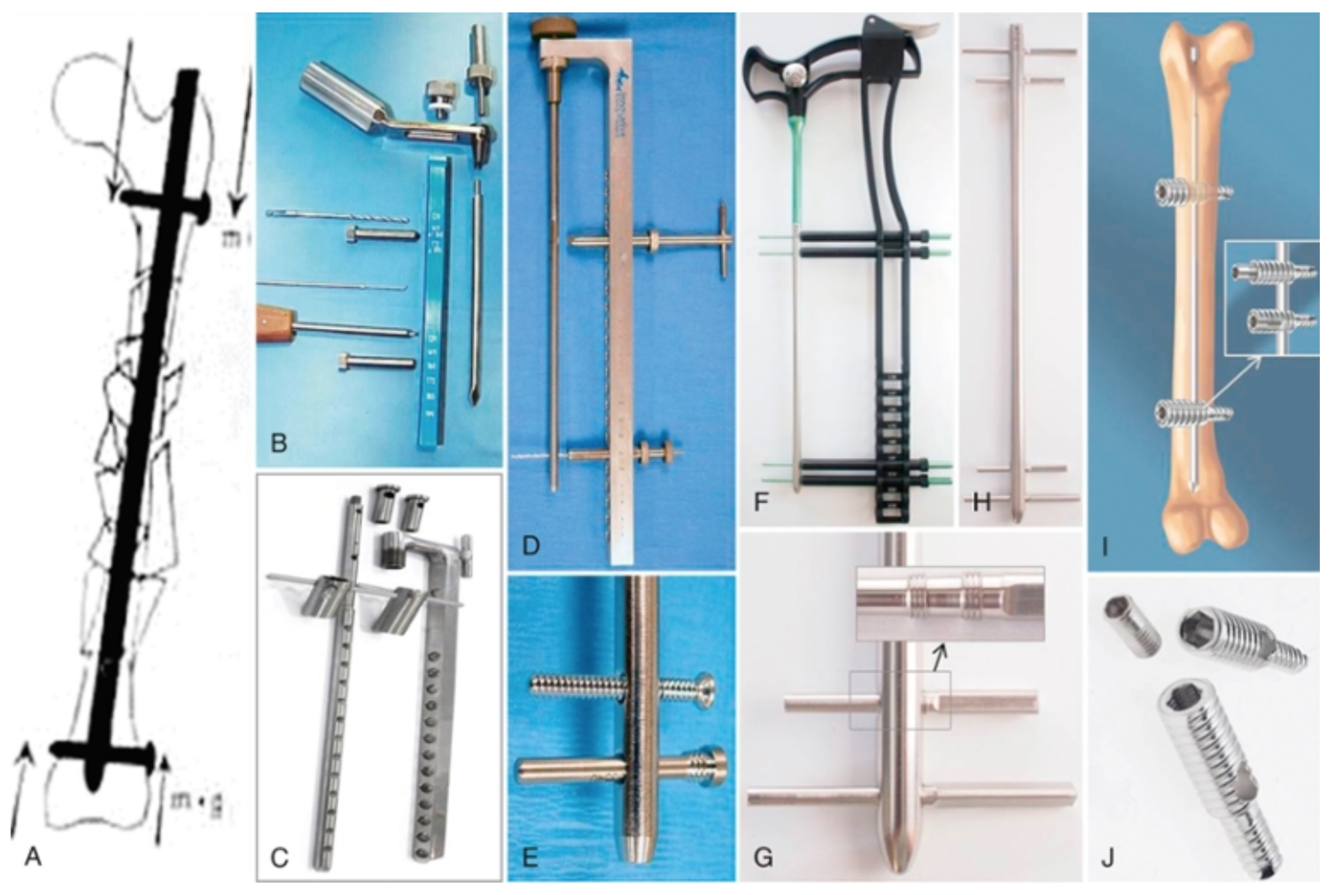
D + E: Regular ILN
F + G: angle stable ILN (iLoc)
I + J: Inverse ILN (Targon)
How is inverse ILN secured?
What is recommended torque?
With a ‘set screw”
1.8 Nm torque
HOw do bolts of regular ILN engage bone?
Threaded portion near head of bolt engages cortex
(Image shows regular ILN screw and bolt, bolts recommended)

What is the locking mechanism of angle stable ILN/bolts?
- Threaded tapered bolts screw into shape matched threaded cannulations in nail (provides rigid nail/bolt interface so cortical threads abolished)
- Morse taper locking screws-cone peg











-
Chapter 38 Tissues of MSK System28
-
Chapter 39 Bone Biomechanics and Fracture Biology38
-
Chapter 40 Open Fractures4
-
Chapter 41 Internal Fixation69
-
Chapter 42 ESF28
-
Chapter 43 Overview of MIO16
-
Chapter 45 Delayed Unions, Non-unions and Malunions5
-
Chapter 46 Principles of Angular Limb Deformity Correction29
-
Chapter 47 Osteomyelitis and Implant-Associated Infections13
-
Chapter 48 Bone Grafts and Substitutes47
-
Chapter 49 Scapula Fractures19
-
Chapter 50 The Shoulder80
-
Chapter 51 Fractures of the Humerus32
-
Chapter 52 Surgical Diseases of the Elbow102
-
Chapter 53 Total Elbow Replacement in Dogs15
-
Chapter 54 Radius and Ulna46
-
Chapter 55 Carpus, Metacarpus and Digits55
-
Chapter 56 Fractures of the Pelvis32
-
Chapter 57 Hip Luxation25
-
Chapter 58 Pathogenesis, Diagnosis, and Control of Canine Hip Dysplasia24
-
Chapter 59 Surgical management of Hip Dysplasia78
-
Chapter 60 Fractures of the Femur86
-
Chapter 61 Stifle STAR WORTHY QUESTIONS ONLY6
-
Chapter 62 Total Knee Replacement in the Dog17
-
Chapter 63 Fractures of Tibia and Fibula19
-
Chapter 64 Tarsus and Metatarsus49
-
Chapter 65 Amputations22
-
Chapter 66 Dentistry for the Surgeon33
-
Chapter 67 Mandibular and Maxillofacial Fractures40
-
Chapter 68 Arthritis42
-
Chapter 69 Misc Ortho Conditions70
-
Chapter 70 Muscle and Tendon Disorders17
-
Chapter 71 Arthroscopy50
-
Chapter 72 Musculoskeletal Neoplasia and Limb Sparing Surgery83
-
Chapter 73 OCD10
