What proportion of shoulder motion comes from the shoulder joint and what proportion from the synsarcosis?
2/3rds from joint
1/3rd from synsarcosis
At what age does glenoid physis fuse?
6 months
At what age does proximal humeral physis fuse?
1 year
What is the ratio of glenoid to humeral head coverage?
What increases the ‘functional’ size of this ratio?
1: 2.5
i. e. moderately congruent.
Cartilaginous glenoid lip increases glenoid joint surface area by 25%
What is approximate thickness of shoulder joint cartilage in 25kg dog?
1 mm
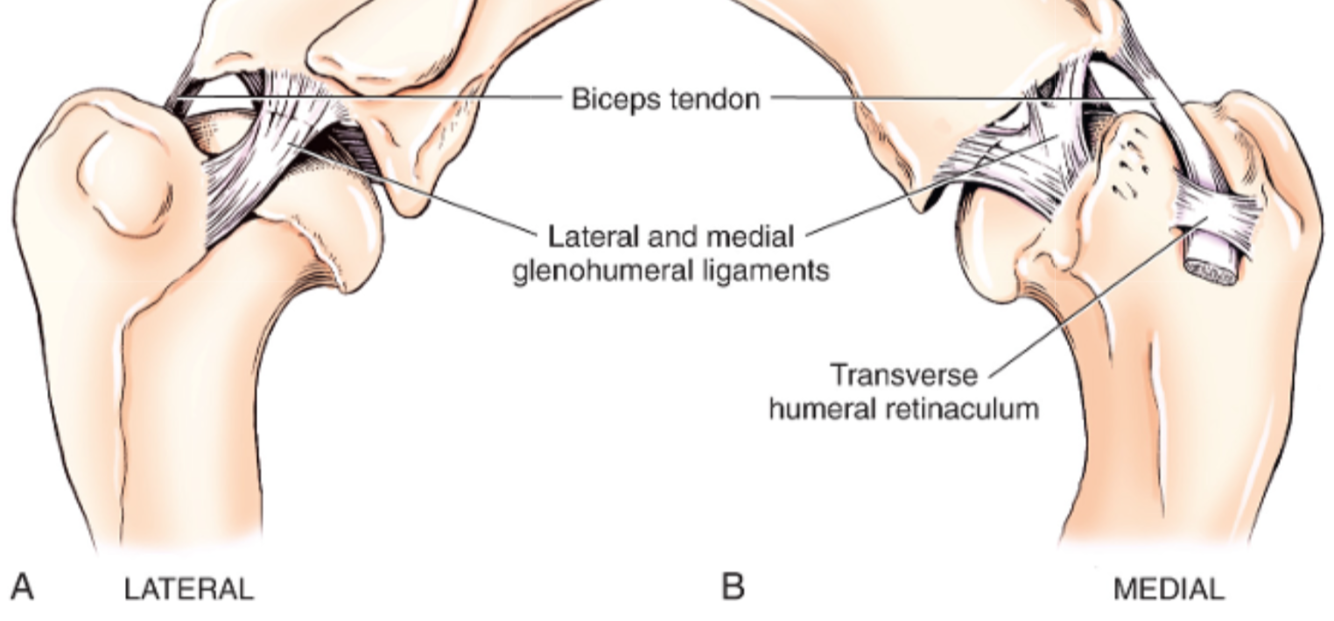
What is the name of the humeral groove through which the biceps runs?
Intertubercular groove
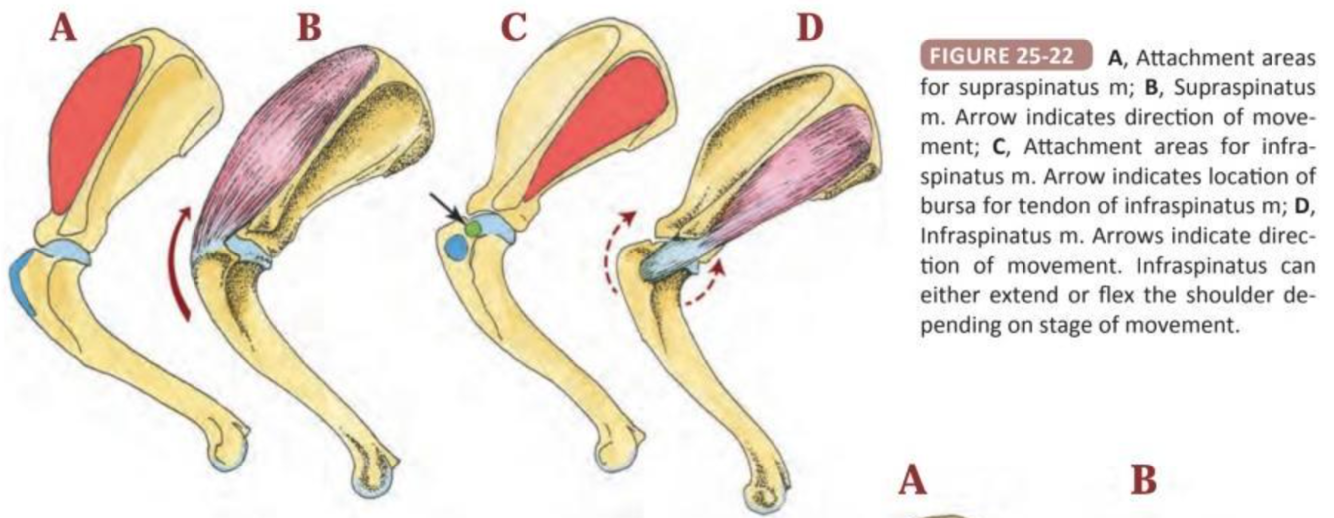
With which 5 muscles does the shoulder joint capsule blend?
- Infraspinatus
- Supraspinatus
- Subscapularis
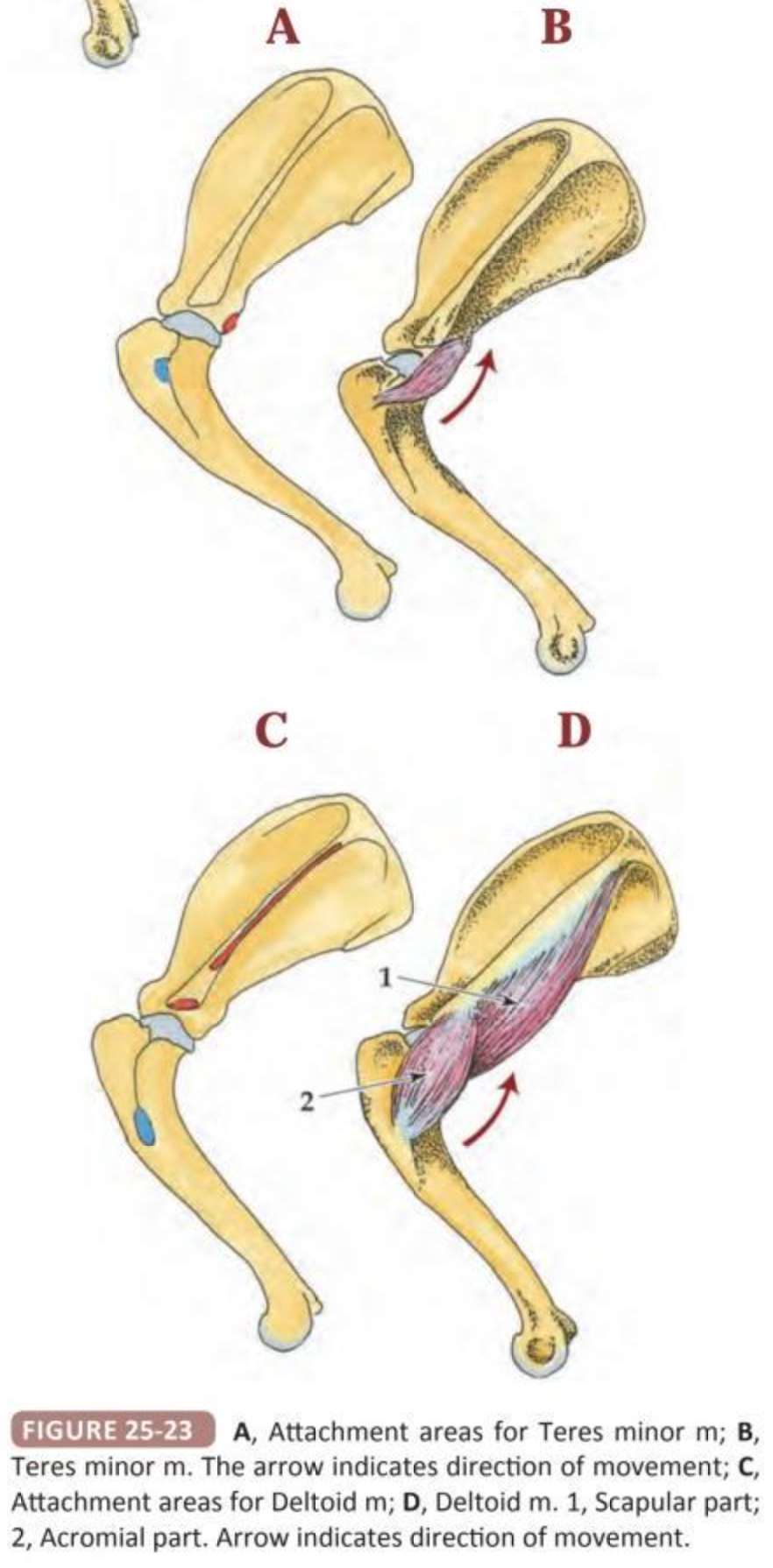
- Teres minor
- Coracobrachialis
Label the diagram
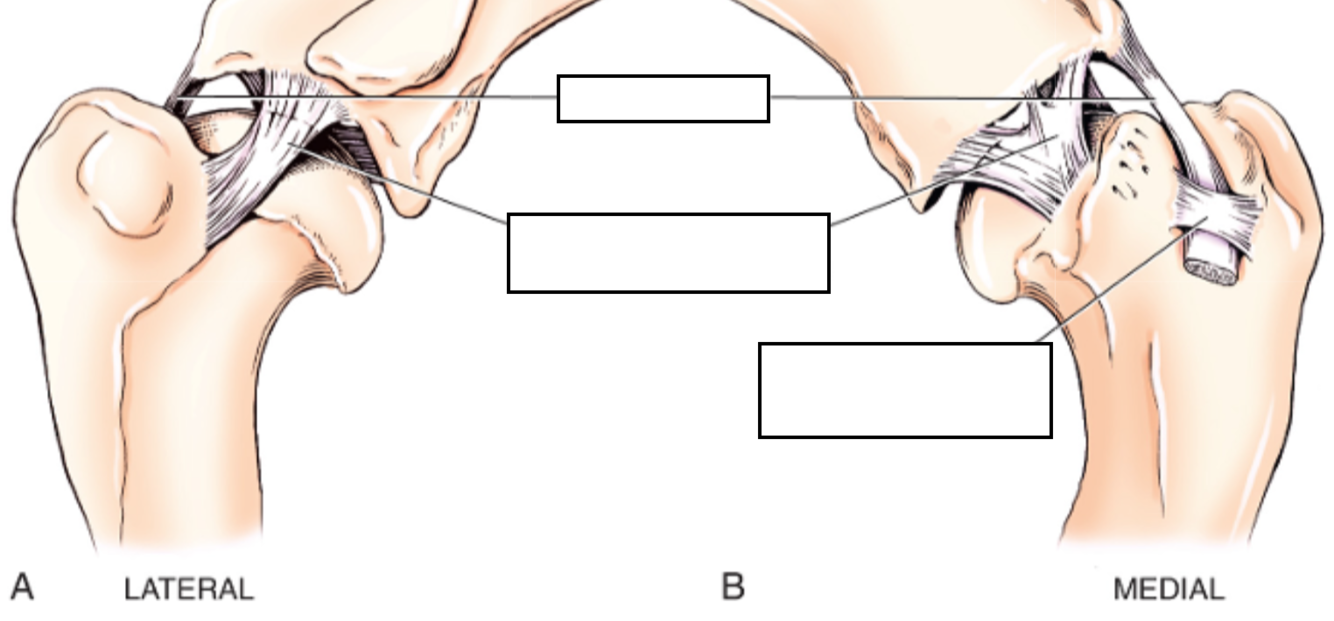
N.B. Cranial arm of Y of exists as separate intra-articular structure
What are normal shoulder joint angles in dog?
And in cat?
What is recommended arthrodesis angle?
Dog:
Flexion 57º
Extension 165º
Cat:
Flexion 32º
Extension 164º
Recommended arthrodesis angle 105 - 110º
List 3 passive stabilisers of the shoulder joint
List 8 active stabilisers of the shoulder joint
Passive shouder stabilisers:
- Limited joint volume + adhesion/cohesion principles
- Concavity compression
- Capsuloligamentous constrainst
- Glenohumeral ligaments
- Joint capsule
- Labrum
- Tendon of origin of biceps brachii
Active shoulder stabilisers
__Major:
- Infraspinatus
- Supraspinatus
- Subscapularis
- Teres minor
Minor:
- Biceps brachii
- Long head of triceps
- Deloideus
- Teres major
Type 1, 2 a dn 3 mechanoreceptors are present in collateral ligaments of shoulder - which type is most common
Type 1 (=Ruffini) receptors
What contrast agent is used fro arthrography?
Iohexol (doent need dilution, unless also performing CT angio in which case dilute to 60 mg/mL
What % of dogs identified by CT as having mineralization of peri-articular structures of shoulder were NOT lame?
40%
And 90% of those with lameness has other shoulder/elbow pathology
i.e. high % of incidental mineralization
What % of shoulder pathology has been reported to be extra-articular (i..e would be missed with arthroscopy alone)?
15%
Name 2 salvage procedures for shouder joint
- Glenoid excision arthroplasty
- Arthrodesis
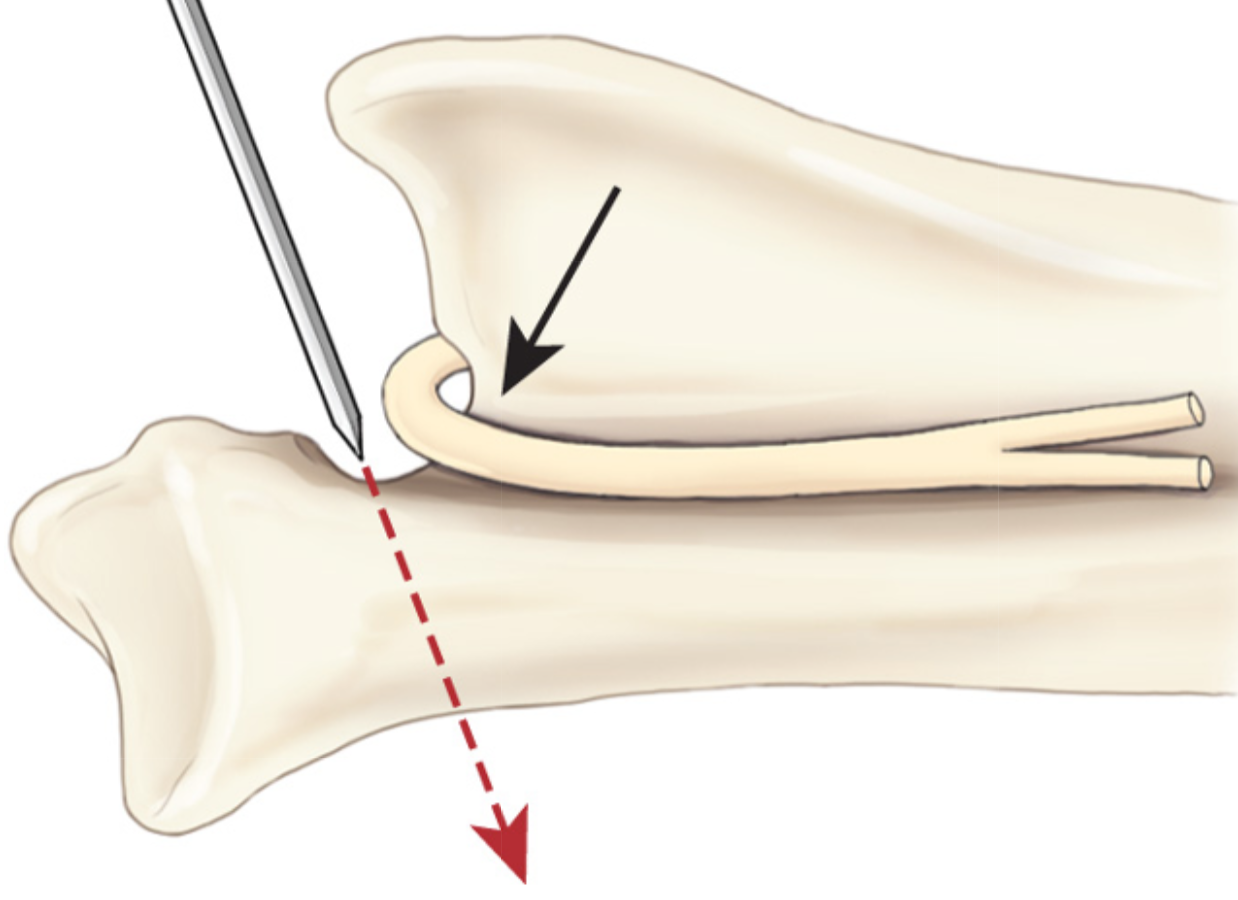
What structure has to be protected/avoided during glenoid excision arthroplasty?
Suprascapular nerve
(also note correct angle of cut: distolateral-proximomedial)
What approach is used for glenoid excision arthroplasty?
Craniolateral
What are the 6 principles of arthrodesis?
What muscle insterts on greater tubercle?
What muscle originates on acromion
Supraspinatus m inserts on greater tubercle
Acromial head of deltoid originates from acromion
i.e. may need to perform ostectomy or tenotomy to allow access to joint
Describe the apprach to perform shoulder arthrodesis
Approach to body, spine and acromion combined with craniolateral approach to shoulder joint (inc tenotomy of acromial part of deltoid, supraspinatus, infraspinatus)
- Elevate insertion of trapezius muscle and origin of the omotransversarius
- The incision is continued distally along the cranial border of the acromial head of the deltoideus muscle.
- The omobrachial vein (and cephalic vein, if necessary) is divided, and the incision follows the lateral aspect of the brachiocephalicus muscle to its insertion.
- The insertion of the superficial pectoral muscle is incised and the muscle elevated and retracted cranially.
- Although osteotomies of the acromion and greater tubercle can be performed, tenotomy of the respective tendons of insertion of the deltoideus and supraspinatus muscles may result in fewer complications due to osteotomy nonunion, if proper hemostasis and reattachment of the muscles is achieved.
- Elevation of the supraspinatus muscle is continued proximally through the entire supraspinous fossa until the muscle can be retracted cranially. The suprascapular nerve is identified, carefully retracted, and protected at all times.
- The tendon of insertion of the infraspinatus muscle is transected and the muscle retracted caudodorsally. This approach exposes the entire craniolateral aspect of the scapula and the cranial aspect of the humerus.
- The lateral collateral ligament is transected and the joint capsule incised to allow luxation of the humeral head from the glenoid fossa.
What are two options for creating a ‘congruent” surface for shoulder arthrodesis?
- Burr cartilage (preferred if normal shape)
- Ostectomy of glenoid + humeral head
What 3 locking plate designs are available?
Name a disadvantage of each
- SOP. Cant generate compression
- LCP: Cant contour in plane
- Reconstruction plate: Can compress but weaker plate
Where is plate placed for shoulder arthrodesis?
How can stabilisation be augmented?
Apply plate along craniolateral scapula and cranial humerus
- Can add ancillary fixation e.g. 2nd plate caudal to first one.
- Or post-op spica splint (possibly innecessary if 2 plates used)
What is recommended shoulder arthrodesis angle?
How else can an arthrodesis angle be derived?
105 - 110º
Compare to opposite shoulder joint angle during weightbearing







-
Chapter 38 Tissues of MSK System28
-
Chapter 39 Bone Biomechanics and Fracture Biology38
-
Chapter 40 Open Fractures4
-
Chapter 41 Internal Fixation69
-
Chapter 42 ESF28
-
Chapter 43 Overview of MIO16
-
Chapter 45 Delayed Unions, Non-unions and Malunions5
-
Chapter 46 Principles of Angular Limb Deformity Correction29
-
Chapter 47 Osteomyelitis and Implant-Associated Infections13
-
Chapter 48 Bone Grafts and Substitutes47
-
Chapter 49 Scapula Fractures19
-
Chapter 50 The Shoulder80
-
Chapter 51 Fractures of the Humerus32
-
Chapter 52 Surgical Diseases of the Elbow102
-
Chapter 53 Total Elbow Replacement in Dogs15
-
Chapter 54 Radius and Ulna46
-
Chapter 55 Carpus, Metacarpus and Digits55
-
Chapter 56 Fractures of the Pelvis32
-
Chapter 57 Hip Luxation25
-
Chapter 58 Pathogenesis, Diagnosis, and Control of Canine Hip Dysplasia24
-
Chapter 59 Surgical management of Hip Dysplasia78
-
Chapter 60 Fractures of the Femur86
-
Chapter 61 Stifle STAR WORTHY QUESTIONS ONLY6
-
Chapter 62 Total Knee Replacement in the Dog17
-
Chapter 63 Fractures of Tibia and Fibula19
-
Chapter 64 Tarsus and Metatarsus49
-
Chapter 65 Amputations22
-
Chapter 66 Dentistry for the Surgeon33
-
Chapter 67 Mandibular and Maxillofacial Fractures40
-
Chapter 68 Arthritis42
-
Chapter 69 Misc Ortho Conditions70
-
Chapter 70 Muscle and Tendon Disorders17
-
Chapter 71 Arthroscopy50
-
Chapter 72 Musculoskeletal Neoplasia and Limb Sparing Surgery83
-
Chapter 73 OCD10
