Define Epilepsy and Seizures
- Epilepsy is a disease characterised by a tendency to recurrent unprovoked seizures
- A seizure is abnormal, excessive synchronised discharge of cerebral neurones
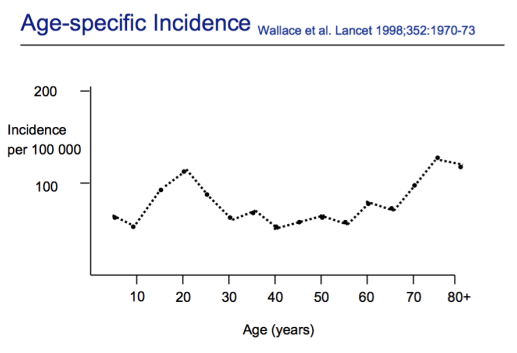
Describe the epidemiology of epilepsy
There are two peaks of incidence of epilepsy. A peak at around 20, and another around 75.
- Thought that the first peak is due to manifestation of genetic condition.
- The second peak is due to neurodegeneration.
Epilepsy is a common disorder. The prevalence of epilepsy = approximately 0.5% (~350,000) in the UK.
- 4th most prevalent neurological condition after migraine, stroke and dementia
- Lifetime risk of epilepsy is 5X higher than either schizophrenia or bipolar disorder
Describe the harms of epilepsy
Epilepsy is not a benign condition, it is quite a dangerous one.
- People with epilepsy: 3-4X more likely to die than age- and sex-matched members of the general population
- 1000 deaths/year in the UK: SUDEP (Sudden Unexpected Death Following Epilepsy), status epilepticus, and injury (drowning is common cause of death of people with epilepsy).
- SUDEP in chronic active epilepsy: 1 in 100 to 1 in 5000 patient years
- Epilepsy and its associated costs >£1bn/year in the UK
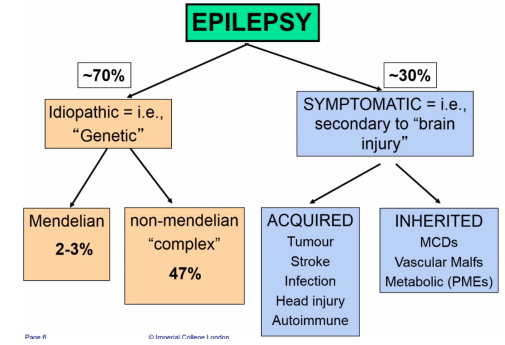
Describe the aetiology of epilepsy
The distribution varies from year to year, but around 70% of epilepsies are due only because the individual has a genetic predisposition towards it, these are called ‘idiopathic’. The other 30% are called symptomatic epilepsies where the condition is a symptom of an underlying brain injury.
- Symptomatic epilepsy arises most commonly as a result of an acquired brain injury from tumour, stroke, infection and head injury, and less commonly, from an inherited brain injury, such as an inherited malformation of cortical development, vascular malformation such as familial cavernomas or metabolic defects such as the inherited progressive myoclonic epilepsies.
- For Genetic epilepsy, only 1 to 2% manifests Mendelian inheritance, with majority having polygenic, non-Mendelian inheritance. There has been considerable success in identifying genes for the rare monogenic idiopathic epilepsies, but this success has not yet been translated into a better understanding of the more common idiopathic epilepsies that do not manifest Mendelian inheritance.
Describe the classifcation of seizures
- Partial (also known as focal seizures). These can be either:
- Simple (does not affect consciousness)
- Complex (does affect consciousness)
- Generalised (begine simultaneously in both hemispheres of the brain). Can be:
- Tonic - rigid muscle tone
- Tonic-clonic - jerky movements
- Absence - loses concentration for a few seconds
- Myoclonic - occasional jerky movement
- Atonic - loss of muscle tone
Describe the genetic influences of non-medelian epilepsy
For the more common genetic epilepsies where there is little/no apparent family history, there are two non-mutually exclusive genetic hypotheses; the rare variant common disease hypothesis and the common variant common disease hypothesis
- The rare variant hypothesis proposes that individually rare (<1%) but highly penetrant variants which can occur in many different genes so that there is an overall high mutation rate to the disease class. This rare variant may be a de-novo mutation.
- Whereas the common variant common disease hypothesis proposes that risk variants confer a low relative risk for the disease, but because these variants are so common (>5% of population) in the population they account for a larger number of cases.
At the moment we don’t know whether common epilepsies are a rare or common variant disease, or a mixture of the two.
Manhattan plots of GWAS. SNPs are single genetic variants. These can be associated with different types of epilepsy. They found that SCN1A, PCDH7 and VRK2/FANCL were associated with development of epilepsy. Shares some loci with schiziphrenia; we now that patients wit epilepsy are at 11x risk of developing schizophrenia.
Describe the role of trio sequencing in discovering de-novo mutations that cause epilepsy
I think what was not expected in epilepsy was the importance of de novo mutagenesis in the severe childhood onset epilepsies. The general approach to discovering genes for a disease by looking for de novo mutation is shown here - this is called the trio design. You take the genetic sequence of the healthy father and mother and compare it to the affected offspring looking at point mutations.
However we can find 1-4 new mutations in every child, and just finding a gene with a protein disturbing de-novo does not necessarily implicate that gene in the disease.
What are the genese implicated in acquired epilepsy?
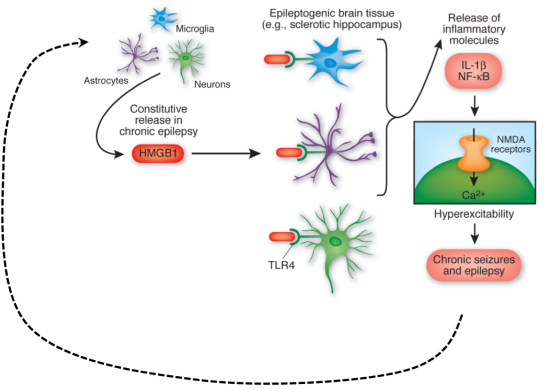
Increasingly we are looking at the role of genetic susceptibility and autoimmunity in acquired epilepsy. There is a role of the innate immune system:
- TLR4 (Toll-like receptor 4) and high mobility group box 1 (HMGB1) are involved in ictogenesis and can be targeted to reduce seizures. There is a constituent release of HMGB1 which binds to TLR4, leading to release of inflammatory molecules such as IL-1B and NF-kB which bind to NMDA receptors causing hyper-excitability.
- This is a positive feedback loop of epileptic seizures leading to more inflammation, then more seizure.
There is also a role of the adaptive immune system in acquired epilepsy:
- Certain autoimmune conditions involve the production of antibodies such as LGI1, CASPR2, NMDAR, GAD, AMPA, GABAA etc..
What are the factors influencing the decision to treat with AEDs (Anti-Epileptic Drugs)?
Anti-Epileptic Drug (AED) Therapy is a balance of BENEFIT and HARM
- Benefits: Seizure reduction, and thus reduction of seizure-related harm.
- Harms: Psychosocial (illness status, self-esteem) Idiosyncratic & dose-related ADRs
Factors influencing decision to treat:
- Number of seizures at presentation. For example, only 50% of people will have another seizure after an first seizure. First seizures are by-enlarge not treated in this country.
- Seizure type and severity
- Cause of seizure
What are the main mechanisms of action of AEDs and give an example for each.
- Enhancing GABA mediated inhibition - e.g. benzodiazepines and barbiturates such as phenobarbital.
- Reducing glutamate-mediated excitation (pre-synaptic) - e.g. levetiracetam and gabapentin
- Reducing post-synaptic glutamate excitation by blocking voltage-gated sodium channels - e.g. parampanel
- Block sodium-channel and thus action potential - e.g. phenytoin, carbamezapine and lamotrigine
- These are quite useful as they block sodium channels in a use-dependent manner. In normal neuronal depolarisation, the drugs do not block the sodium channel. But in the fast and repetitive action potentials seen in a seizure, the drugs act to block the sodium channels.
Describe the MoA of benzodiazepines
Benzodiazepines such as diazepam and lorazepam work by increasing frequency of GABAA opening and increasing affinity for GABA binding.
Increased GABA binding = increased Cl- inside cell, and increased polarisation –> less excitation.
Describe the MoA of barbituates
Barbiturates such as phenobarbitol work by increasing duration of Cl- channel opening, increasing affinity for GABA binding and in high concentrations can directly stimulate Cl- channel.
Describe the MoA of Levetiracetam
Levetiracetam, is a pyrolidone derivative licensed in the UK 2001. It was initially developed in the 1980s as a drug with cognitive enhancing effects but early trials were unsuccessful and so it was tried in epilepsy. It is now among the most promising of the new antiepileptic drugs, but its mechanism of action is completely unknown. In the past 12 months there have been papers claiming 3 different mechanisms of action.
Thought to bind to the vesicular protein SV2A to prevent the release of excitatory neurotransmitters.
Describe the MoA of Gabapentin
First licensed in 1993, it was synthesised to have a close structural relationship to GABA, from where it derives its name. When first released, it was marketed as a GABAergic drug. It now appears the binding site for gabapentin in fact the alpha 2 delta subunit of the pre-synaptic voltage gated calcium channel. Rather than enhance GABA, gabapentin is now thought to mediate its anticonvulsant effect by inhibiting the release of glutamate and other neurotransmitters from the presynaptic neuron.
Describe the MoA of parampanel
Reducing post-synaptic glutamate excitation by blocking voltage-gated sodium channels.
Describe the MoA of phenytoin, carbamezapine and lamotrigine
Block sodium-channel and thus action potential.
These are quite useful as they block sodium channels in a use-dependent manner. In normal neuronal depolarisation, the drugs do not block the sodium channel. But in the fast and repetitive action potentials seen in a seizure, the drugs act to block the sodium channels.
