Here is a histologic sample of the cervix of a sexually active young woman. What is notable about the sample?
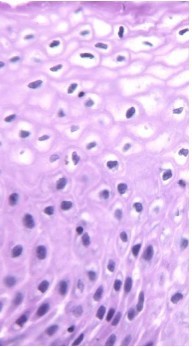
Cervical dysplasia:
Koilocytes from HPV infection: HPV has invaded basal cells. Crinkled, irregular nuclei with “normal maturation” of cells.
First AID:
- CIN 1, 2, or 3 (severe dysplasia, carcinoma in situ)
- Associated with HPV 16– E6–> inhibits p53 or HPV18–> E7–> inhibits Rb
- *Risk factors**: #1= multiple sexual partners
- Smoking, early sexual debut, HIV infection
A woman presents to your office for a pap smear after not having one for 10 years. She noticed some bleeding and discomfort with intercourse. Upon exam, you find the following:
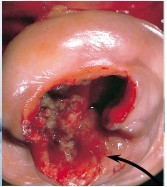
Invasive cervical carcinoma
Fully invasive carcinomas are exophytic/ ulcerating, and can be keratinizing or non-keratinizing.
- Can invade adjacent structures (parametrium, bladder, rectum) causing ureter obstruction (–> renal failure) and fistula formation. - Lymph spread to paracervical, hypogastric, external iliac lymph nodes
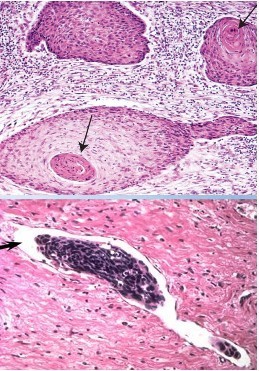
Endometriosis
- *Endometriosis**:
- Non-neoplastic endometrial glands/stroma in abnL location outside utereus (may be due to retrograde menstrual flow)
- Ectopic endometrial tissue= Chocolate cysts (blood) in ovaries; red/blue punctate lesions on bladder mucosa; painful defecation during menstruation (in pouch of Douglas)
- NORMAL uterus size
Symptoms:
- Severe menstrual-related pain
- Painful intercourse, infertility
Tx: Oral contraceptives, NSAIDs, leuprolide (GnRH agonist), danazol (modified progestin)
- *Adenomyosis**= endometrium within myometrim–> enlarged uterus, menorrhagia, dysmenorrhea, pelvic pain
- Tx: hysterectomy
A 60 year-old woman presents with post-menopausal bleeding. You perform an endometrial biopsy and find the following cell types:
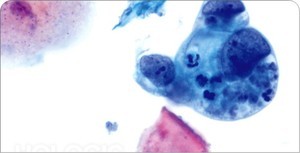
Endometrial carcinoma:
FIRST AID:
Most common gynecological malignancy
- Peak at 55-65 years
- Presentation= vaginal bleeding (typically preceded by endometrial hyperplasia)
Risk factors:
- estrogen (w/o progestin): nulliparity, late menopause
- Obesity, diabetes, HTN
Increased myometrial invasion–> worse prognosis
Endometrial adenocarcinoma: 70% present at stage 1, surgery is sufficient for treatment. 5-year 96% survival with no metastases vs 66% with metastatic spread
Endometrial lining connects to vagina- presents early. ANY post-menopausal bleeding needs to be worked up (~10% associated with endometrial cancer)
Screening: transvaginal sonography; unable to complete meaningful endometrial stripe measurement. Not used for evaluating asymptomatic patients.
Diagnosis: dilation and curettage, endometrial biopsy, hysteroscopy (small camera inside uterus)
Treatment: surgery, radiation (whole pelvic or brachytheraphy= vaginal area), oral progesterone (high failure rate), chemotherapy (only in high-grade serous tumors like ovarian cancer)
Prognosis: 85% five-year survival
* Re-screen patients who have repeated bleeding within 3 months of first evaluation
Leiomyoma
- *Leiomyoma**:
- Most common of all tumors in females
- Benign smooth muscle tumor(s) in uterus
- RARE malignant transformation (Leiomyosarcoma usually arises denovo and is highly aggressive)
Estrogen sensitive: increases with pregnancy, regresses with menopause
Symptoms:
- asymptomatic–> abnL uterine bleeding–> miscarriage
- Severe bleeding–> iron deficiency
Histo: whorled pattern of smooth m.
An obese 28 year-old woman goes to a fertility clinic complaining of problems of conceiving after trying for 16 months. She states she has never had regular periods. She has acne and her fasting blood sugar is elevated. An ultrasound of her uterus and ultrasound is performed and the following image is taken. What is her diagnosis and treatment?
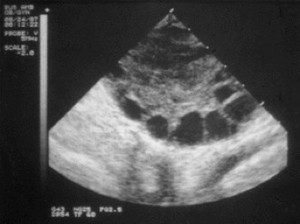
PCOS: polycystic ovarian syndrome. The patient has cytic ovaries, hirsutism (acne), is overweight, and shows some level of insulin resistance.
7% women affected by PCOS (leading cause of infertility): see cystic follicles, atresia, and persistant anovulation; hirsutism, acne, male-pattern alopecia, obesity
Labs:
- Increased LH, decreased FSH
- Increased Testosterone–> aromatization lead to increased estrogen levels
Treatment
- Weight reduction
- Low-dose OCPs (progesterone supplementation)
- Medoxyprogesterone–> decreased LH and androgenesis
- Spironolactone= blocks androgens (for acne, hirsutism)
- Clomiphene= SERM–> prevents estrogen from negatively inhibiting hypothalamus–> increased gonadotropin production (FSH, LH)–> ovulation

A 26 year old woman comes to her physician complaining of bleeding in between periods. She ovulates every month (she has been watching her cycles as she prepares to get pregnant) but is concerned about this bleeding. Ultrasound reveals a cyst in one of her ovaries. What type of cyst is it?
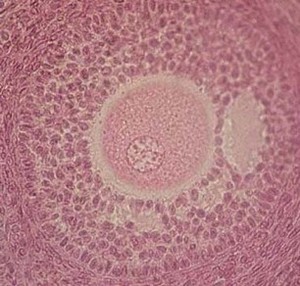
Ovarian cyst: arises from surface epithelium (cortical inclusion) or from ovarian follicles (follicular/corpus luteum cysts). Asymptomatic, may see precocious puberty, menstrual dysfunction, rupture
- *1. Follicular cyst=** Unruptured graafian follicle. Most common ovarian mass in young women
- Hyperestrinism
- Endometrial hyperplasia
Corpus luteum cyst: delayed resolution of corpus luteum–> increased progesterone production–> menstrual irregularities
Theca lutein cysts (hyperreactio luteinalis): high gonadotropin levels–> multiple/bilateral cysts–> can rupture, leading to intraabdominal hemorrhage (associated with choriocarcinoma and moles)
* Can see virilization in 15% of affected women (elevated progesterone–> hirsutism)
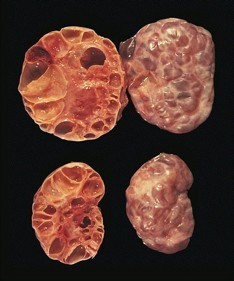
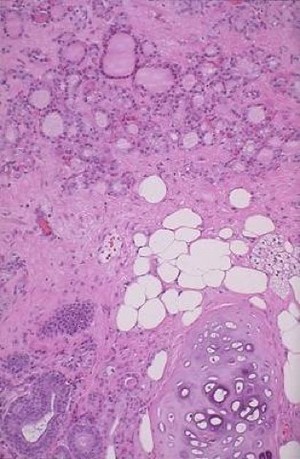
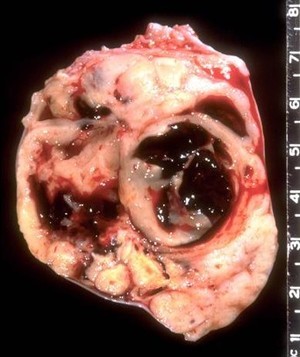
Below is a specimen recovered from an ovary. What type of tumor is this and what is the prognosis?

Dermoid cyst- mature teratoma
Ovarian germ cell teratoma: see somatic differentiation within germ cell. This is a mature teratoma (recovered from ovaries- therefore germ cells) and is much more likely to be benign. An immature teratoma is found in other tissues, is composed of embryonic tissue and is malignant (totipotent cells with 3 germ layers)
Though benign, these tumors grow other cell types within them that can transform into malignancy (ex. skin can lead to squamous cell carcinoma, or thyroid tissue can lead to papillary thyroid carcinoma)
Below: teratoma with adipose and thyroid papilary tissue
Endometrioid cyst
Endometriosis within ovary–> cyst formation
- Varies with menses
- Chocolate cyst= filled with dark blood
Ovarian germ cell tumors
Most common in adolescents
- *Dysgerminoma= malignant, rarer than male seminoma (hCG, LDH** producing)
- Sheets of uniform cells
- Associated with Turner’s syndrome
Choriocarcinoma= rare, malignancy of trophoblastic tissue
- NO chorionic villi
- Increased frequency of theca-leutein cytst
- Can derive from moles or post-partum in mother or babcy
- Elevated hCG- can mimic TSH–> hyperthyroidism
- Hematogenous spread to lungs
Yolk-sac (endodermal sinus) tumor= aggressive malignancy in ovaries, sacrococcygeal area of young children
- Yellow, friable solid masses
- 50% have Schiller-Duval bodies (resemble glomeruli)
Teratoma: 90% of ovarian germ cell tumors
- 2-3 germ cell layers
- Mature= dermoid, benign
- Immature (2 layers); aggressively malignant
- *Struma ovarii:** functional thyroid tissue–> hyperthyroidism
Below is a sample from the ovary of a 60 year old woman with no children and a family history of breast cancer (sister at age 45, mother at 53). What is the abnormality below and what is the prognosis?
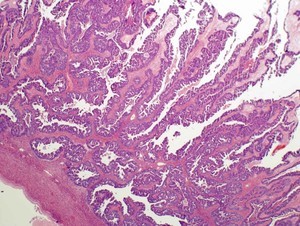
Serous cystadenocarcinoma
- 45% of ovarian tumors (other 45% benign cystadenoma)
- Malignant, bilateral
- Psammoma bodies (calcifications) on histology
- *Risk factors**: BRCA-1, BRCA-2, HNPCC
- Genetic predisposition: family history most important risk factor
- *Vs serous cystadenoma**: 45% of ovarian tumors; bilateral, fallopian-tube like simple ciliated columnar epithelium
- Benign
- Increased CA-125 (marker for ovarian cancer)
Mucinous cystadenocarcinoma
- *Mucinous cystadenocarcinoma**:
- Malignant
- Pseudomyxoma peritonei= intraperitoneal accumulation of mucinous material from ovarian or appendiceal tumor
Histo: ceolomic/germinal epithelium dervied–> produces mucin
Brenner tumor
- *Brenner tumor**:
- Benign, unilateral
- Resembles bladder: pale yellow-tan, encapsulated
- “Coffee bean” nuclei on H&E
Below is a benign ovarian tumor removed from a 60 year old woman. She was diagnosed with this tumor due to increasing ascites/pleural effusion before it was removed but since removal her symptoms have resolved. What type of tumor is this and what was her diagnosis?

Benign fibroma= 75% of stromal tumors, associated with Meig’s syndrome= ovarian fibroma, ascites, hydrothorax (tumor causing ascites). Solid white tissue.
Benign thecoma (below)= similar to fibroma, may produce estrogens/androgens, causing systemic effects. Fatty yellow tissue.

Below is a sample from an ovarian tumor removed from a post-menopausal woman. Before diagnosis, the woman presented with endometrial bleeding. What type of tumor is in the histologic sample below?
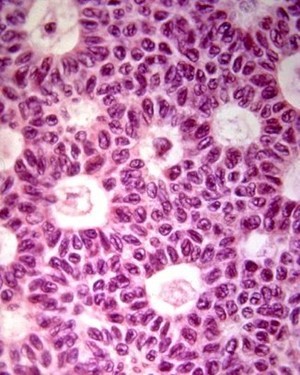
Granulosa cell tumor (post-menopausal adult form): presents with Call-Exner _body, an estrogen-producing cluster of cells with grooved nucle_i (causing endometrial thickening/hyperplasia).
Cystic, hemorrhagic tumor (see below)
Juvenile form seen in children and young women causing precocious puberty and hyperestrinism
Krukenberg tumor
Krukenberg tumor: GI malignancy metastasizes to ovaries
–> mucin-sectreting signet cell adenocarcinoma
Fibroadenoma
- *Fibroadenoma**: BENIGN
- Stromal tumor
- Small, mobile, firm mass with sharp edges
- MOST common tumor in women < 35 years
- Estrogen-sensitive: increased size, tenderness with pregnancy, menstruation
- NOT precursor to breast cancer
Intraductal papilloma
- *Intraductal papilloma**:
- small tumor growing in lactiferous ducts
- Beneath areola
- BENIGN (v. small increased risk in carcinoma)
Symptoms: bloody or serous nipple discharge
Phyllodes tumor
- *Phyllodes tumor**:
- Large bulky mass of conective tissue and cysts in stroma
- Leaf-like projections
- Most common in 6th decade
- BENIGN- but, some risk for malignancy
Ductal carcinoma in Situ (DCIS)
- *Ductal carcinoma in situ**:
- Fills ductal lumen
- Ductal hyperplasia (major duct)
- No basement penetration (penetrates–> invasive ductal carcinoma= most common)
Comedocarcinoma
- *Comedocarcinoma**:
- Ductal tumor
- Caseous necrosis (central necrosis with cancer cells around)
- Subtype of DCIS
Invasive ductal carcinoma
- *Invasive ductal carcinoma**:
- Firm, fibrous, rock-hard mass with sharb margins
- Small, glandular duct-like cells
- “Stellate” morphology
- worst, most invasive, most common (76% of all breast cancers)
Invasive lobular cancer
- *Invasive lobular cancer**:
- Orderly row of cells “Indian file”
- Bilateral with multiple lesions in same location
Medullary breast cancer
- *Medullary breast cancer**:
- Fleshy, cellular, lymphocytic infiltrate
- Good prognosis














-
Microbiology186
-
Microbiology pharm63
-
Endocrine69
-
Genetics, Biochem138
-
Anatomy5
-
Hematology/oncology109
-
Cardiac103
-
Behavioral science42
-
Immunology81
-
Renal60
-
Renal patho29
-
Pulmonology43
-
Pulm Path20
-
Embryology34
-
Repro39
-
Repro path38
-
Pharmacology basics59
-
Random cards41
-
Neuro133
-
Neuro path30
-
GI path112
-
GI74
-
Endo Pathology52
-
Musculoskeletal Path111
-
Derm/Musculoskeletal63
-
Psych50
