in cardiac wall - which is the OUTER and INNER layer?
what cells compromise the myocardium?
inner: endocardium - inside is blood / heart chamber
outer: epicardium
Myocardium: Comprised of cardiac myocytes, interlinked with intercalated discs with gap junctions on them. These myocytes are supported by fibro-collagenous tissue with extensive vascularisation
which cardiac layer are purkinje fibres in?
a) epicardium
b) myocardium
c) endocardium
d) subendocardium?
which cardiac layer are purkinje fibres in?
a) epicardium
b) myocardium
c) endocardium
d) subendocardium
what are the three layers that make up the heart valves?
– Fibrosa: forms the core of the valve -DIC.
– Spongiosa: LCT on atrial side (loose collagen/elastic fibres), as shock absorber. has bubble morphology (looks like a sponge)
– Ventricularis: Adjacent to ventricular surface of the valve. DCT with elastic fibres. Forms the chordae tendineae (fibrous cords covered with endothelium).
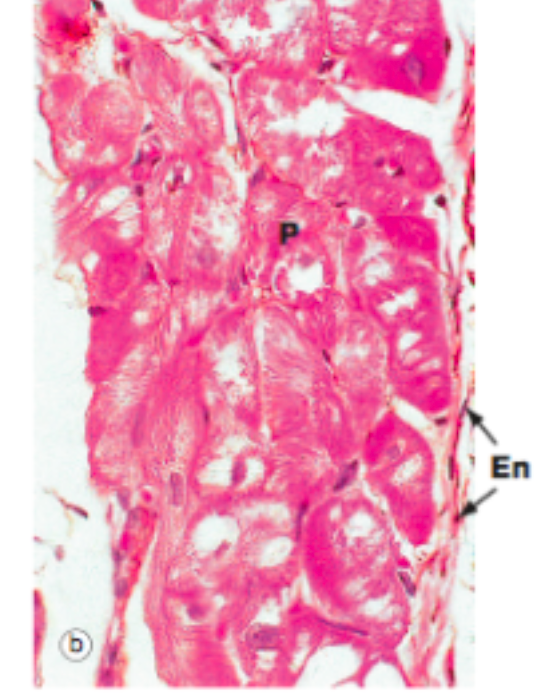
purkinje fibres conduct depolaristion of heart. they’re sepcialised myocytes. How are they different to normal myocytes found in the myocardium?(4)
- are larger than cardiac muscle fibres
- have central pale staining with most of the common red staining shown in the periphery of the cell. - no T-Tubule system and
- connect with each other via desmosomes and gap junctions rather NO intercalated discs.
where do u find discontinous capillaries? why ?
what does this describe: ‘contractible cells wrapped around the endothelial cells’ - what is their function?
thymus & spleen - to allow leukocytes to leave !
= pericytes -> produce fibroblasts
what are valves made from
valves: are semilunar projections of tunica intima into the lumen of the vessel. A
where do you find each of the following:
a) fenestrated capillaries
b) continous capillaries
c) discontinous capillaries
a) fenestrated capillaries: extensive molecular exchange with the blood such as the small intestine, endocrine glands and the kidney.
b) continous capillaries: muscle & nerve tissue
c) discontinous capillaries: liver, thymus and spleen - that allows proteins, or even blood cells to pass through.
what is pressure in sysetmic and pulmonary circ? at normal levls
systemic circ:
a) normal: 120 /80 mmHg
pulmonary circ:
a) normal: 25/8 mmHg
what is starlings law of the heart?
- ventricular contractile force is proproportional to end diastolic volume (aka ventricle will pump out however much blood is delivered to it by atria - more blood: more strongly pumped)
- if more blood is delivered: ventricle expands to a greater diameter & contracts more strongly
why?
at low EDV: there is less overlap of cross bridges (of actin and myosin): weak contraction
at high EDV: more overlap of cross bridges stronger contraction
ncreasing the overlap of active region of A & M increases the force of contraction
BUT limit to starlings law:
- If the preload is too great and the ventricle expands beyond a certain volume, the mechanism fails: ventricle contracts more weakly
- this is a tipping point: beyong which heart failure starts to occur
what is cardiac output? - what is it a product of?
and what is stroke volume? what is SV in normal, healthy person?
what is end diastolic volume? what is end systolic volume? why different?
how do u work out stroke volume from EDV and ESV?
- *cardiac output:** is the amount of blood pumped by the heart minute (litres / min)
- product of heart rate (HR) and stroke volume (SV)
stroke volume: volume of blood ejected during ventricular contraction or for each stroke of the heart. usually 70ml
- *EDV** is the filled volume of the ventricle prior to contraction
- *ESV** is the residual volume of blood remaining in the ventricle after ejection (not all gets ejected)
stroke volume = EDV - ESV (e.g EDV: 120 ml - ESV: 50 ml =70ml)
what is isometric contraction of the ventricles?
Isometric contraction is when the pressure is rising in the ventricles, yet not enough for the aortic/pulmonary valves to be pushed open.
what are the lubb and dupp heart sounds caused by? aka?
lubb: closure of AV valves followed by the opening of the aortic and pulmonary artery valves is the first heart sound. This is known as S1.
dupp: closure of the aortic and pulmonary artery valves followed by the opening of the AV valves is the second heat sound, known as S2
what are s3 and s4 sounds? which pops more likely to hear?
what botth caused by?
- *S3:
- ** faint low-pitched sound is heard in about 1/3 of the way through diastole in many children and young adults.
- period of rapid ventricular filling and is due to turbulent flow during the filling
- a sign of serious heart damage, possibly damaged heart valves.
- *s4:**
- *-** sometimes heard immediately before the first heart sound.
- It is due to turbulent flow in the ventricle and rarely occurs in normal adults.
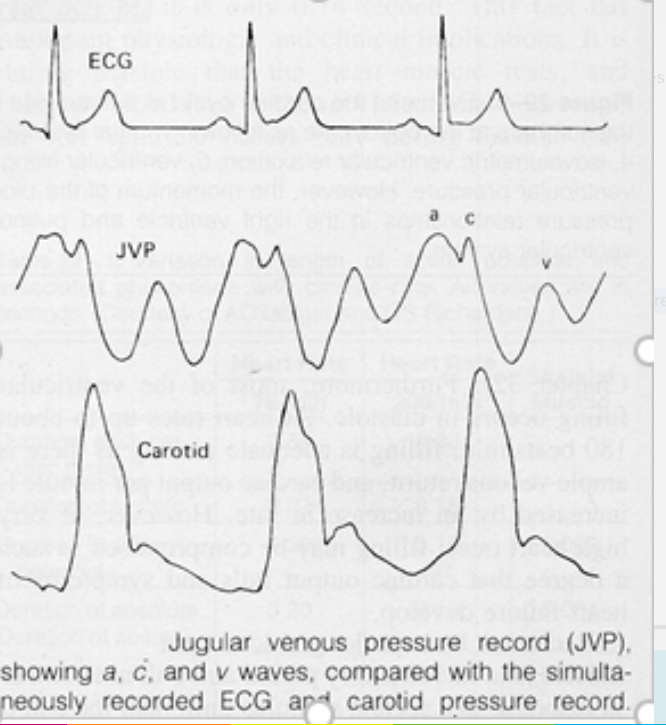
what is JVP? what are the 3 waves of it
the jugular venous pulse: right atrium contracts a back pressure that occurs in the jugular vein
There are three peaks in the venous pulse: a, c, and v:
- a pulse is due to atrial contraction just before the tricuspid valve closes
- c wave is due to pressure rising in the atrium just after the tricuspid valve closes before the valve bulges back into the atrium,
- v wave corresponds to venous filling when the tricuspid valve is closed
Venous return to the heart is mediated by which three main factors?
One way valves in the veins
Muscular pumps
Thoraco-abdominal pump. During inspiration, pressures in the thoracic cavity are reduced, pulling blood into the inferior vena cava. On exhalation, thoracic pressure increases and this blood is forced into the right atrium
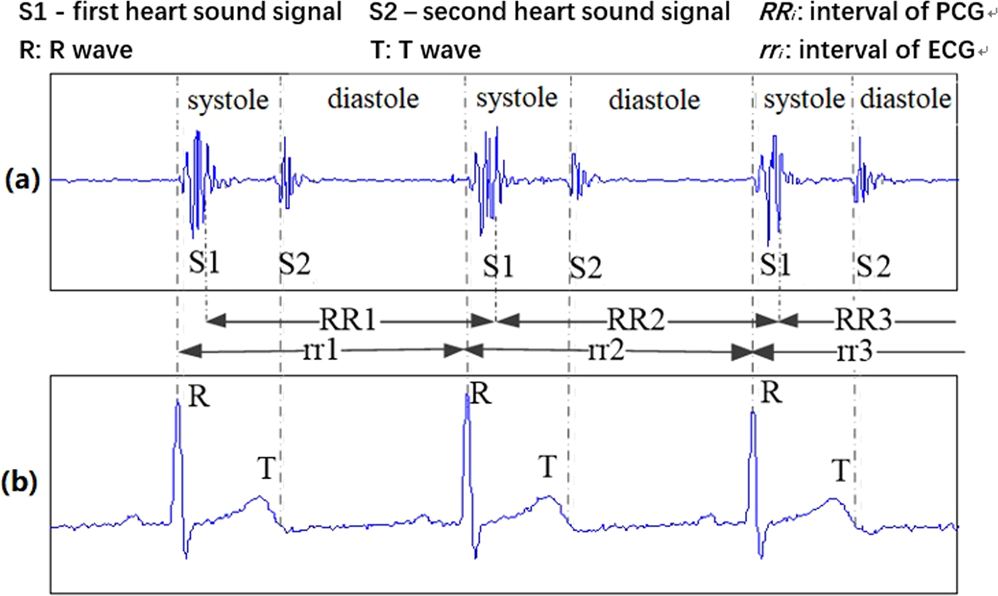
when doe S1 and S2 heart sounds corresspond to on ECG?
Heart sounds:
- *LUBB / SI:** after QRS
- *DUPP / S2:** after T phase
Q
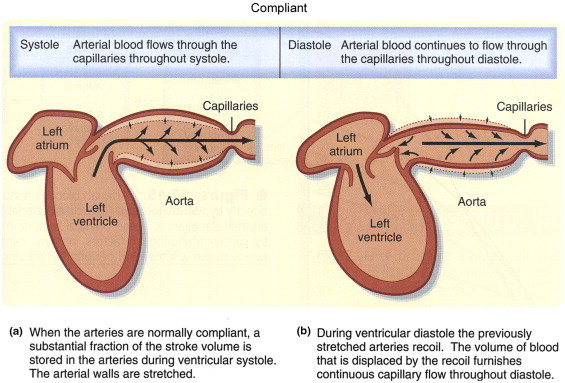
what is the Windkessel effect?
The walls of the aorta and elastic arteries distend when the blood pressure rises during systole and recoil when the blood pressure falls during diastole. There is a thus net storage of blood during systole which discharges during diastole.
Without this distension and recoil they would easily become damaged when the pressure rises, and their ability to accommodate the rapid blood flow is beneficial for keep pressure high
how
Pulse pressure is the difference between systole and diastole. As arteries are elastic, pulse pressure normally decreases slightly from aorta to brachial artery
Mean arterial pressure (MAP) is calculated as diastolic plus 1/3 pulse pressure
what happens to diastolic and systolic pressure when have stiff arteries?
what effect does this have on LV afterload and myocardial oxyegen demand?
there is a decrease in diastolic pressure (& increase in systolic presure)
These changes in pressure components increase LV afterload and myocardial oxygen demand
how much ml per minute of blood does the following need?
brain, heart & kidneys?
what % do these three take up of overall cardiac output?
Your BRAIN needs about 700 ml per minute of blood (14-15% resting Cardiac Output)
Your HEART needs about 200 ml per minute of blood (4% resting cardiac output)
Your KIDNEYS take about 1250 ml/min (25% resting cardiac output)
These three organs take up about 40-45% C.O at rest.
Which two factors influence the work of the heart? !
- Diameter of arterioles (main)
- Viscosity of blood
what influences viscosity of blood? (4)
blood viscosity depends on:
1. (mainly) on the haematocrit (proportion of red cells in blood, normally ~45%
2. On the mechanical properties (mainly the deformability) of the red cells:
If the cells are too large or malformed (e.g. as in sickle cell disease) they clog up the capillary and oxygen delivery is compromised
3. red blood cell aggregation
4. plasma viscosity.
Q
what is polycythaemia? what is absolute polycythaemia? what is relative polycythaemia?
A
Polycythaemia is a disease state in which the haematocrit increases. It can be due to an excessive production of red blood cells, absolute polycythaemia, or to a decrease in the volume of plasma, relative polycythaemia
what are immature RBC called?
what stain used?
how do RBC make ATP - what does mean for pH?
- reticulocytes
- methylene blue
- RBC produce ATP by glycolysis (glucose -> pyruvate -> lactic acid)
- due to lactic acid = low pH


-
The Mediastinum27
-
CR Anatomy: Question Bank17
-
The Heart and Coronary Arteries34
-
Clinical Skills: CV1
-
The Conducting System of the Heart & ECG43
-
Anatomy: Practical 1 - Mediastinum43
-
Smooth and Cardiac Muscle32
-
CVS Histology48
-
Anatomy: Practical 2 - Thorax and the Lungs41
-
Heart as a Pump40
-
Haemodynamics35
-
Carriage of Oxygen in the Blood24
-
Review of the Sympathetic Nervous System34
-
Neural Control of Blood Pressure28
-
Renal Function 128
-
Renal Function 227
-
Blood volume & pressure control after Haemorrhage0
-
Microcirculation & Oedema35
-
Microanatomy - Histology of Hematopoietic System29
-
Peripheral Vasculature of the Limbs39
-
Drug Treatments for CVD24
-
Anatomy of the respiratory system27
-
Hormonal Control of BP32
-
Introduction to Respiratory System29
-
Anatomy of the upper airway41
-
Anatomy: Practical 2 - Thorax and the Lungs (Part 2)36
-
Pulmonary Circulation25
-
Chest X-rays28
-
Respiratory Physiology I17
-
Respiratory Physiology II25
-
:)51
-
Histology of Resp. System34
-
Pharmacology of the Airways14
-
Histology Qs7
-
Acid-Base Control of Respiration28
-
Gas Exchange and Lung Function Tests27
-
big boys29
-
::)53
-
:O50
-
:L54
-
:D13
