the Fick Principle says that:’ The volume of gas which diffuses per unit time across a tissue sheet is…. ‘
(4)
what makes gas transport maximised in the lungs? (4)
- Proportional to the area of the sheet
- Inversely proportional to the thickness of the sheet
- Proportional to the difference in partial pressure of the gas on the two sides
- Dependent upon the permeability coefficient* for that gas in the tissue
We maximise gas transport in the lungs by having a large exchange area, a thin diffusion membrane, a high partial pressure difference, and a high permeability coefficient
According to the Fick principle, gas transfer from alveoli to capillaries is reduced when there is: (4)
- Reduced surface area, e.g. in pneumonectomy, lobectomy or reduced ventilation from airway obstruction or reduced effective area with emphysema or increased dead space
- Increased thickness of alveolar membrane with pulmonary fibrosis, alveolar proteinosis, and acute lung injury
- Reduced oxygen concentration, as in high altitude
- Inadequate time for gas transfer, if there is lung disease
The average partial pressure of oxygen in the alveolar gas is ~ ?? mm Hg
how is this different when not looking at averages? (i.e. at base and apical alveolar gas)
The average partial pressure of oxygen in the alveolar gas is ~100 mm Hg
BUT
Ventilation perfusion mismatch:
- apex alveoli gas = higher partial pressure, close to tracheal levels of 150 mm Hg.
- lung base alveoli in the lung bases conversely has a much lower partial pressure of oxygen.
Typical values would be:
Apical alveolar gas; 135 mm Hg
Basal alveolar gas; 92 mm Hg
what is the PaO2 difference in alveolar membrane and pulmonary venous blood? what is pressure difference? what does this mean?
what is PaCO2
- PaO2 in mixed pulmonary venous blood: about 45 mm Hg
- PaO2 alveolar membrane: 100 mm Hg
- partial pressure difference driving oxygen into the first parts of the pulmonary capillaries is about 55 mm Hg. (100 - 45) Because of the efficient transfer, by the time the blood has reached the end of the pulmonary capillaries the partial pressure in the blood has risen to ~95 mmHg, nearly the alveolar level.
- PaCO2 in mixed pulmonary arterial blood: about 46 mm Hg
- PaO2 alveolar membrane: **40 mm Hg
- difference:6 mm Hg**
SO Changing the breathing rate WILL affect the excretion of CO2.
why does changing the breathing rate at rest not normally affect the arterial oxygen saturation?
Hb is effectively saturated with oxygen even if the partial pressure in the pulmonary capillary blood is as low as 80 mm Hg - so there is a high safety factor for oxygen uptake
what happens when you hyperventilate to oxygen and co2 uptake?
When you hyperventilate a healthy lung, you do not effect oxygen intake yet you do effect CO2, as CO2 can easily be breathed out via hyperventilation
During hyperventilation the rate of removal of carbon dioxide from the blood is increased. As the partial pressure of carbon dioxide in the blood decreases, respiratory alkalosis, characterized by decreased acidity or increased alkalinity of the blood, ensues. I
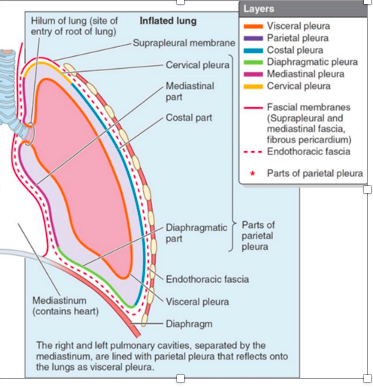
What keeps the lungs kept ‘glued’ to the inside of the thoracic wall? (2)
(1) The intra-pleural fluid cohesiveness:
- water molecules in the intra-pleural fluid are attracted to each other and resist being pulled apart
- *=** pleural membranes tend to stick together
(2) The negative intra-pleural pressure:
- the sub-atmospheric intra-pleural pressure creates a pressure gradient between the lung wall and the chest wall. This holds the outer surface of the lung against the inner surface of the thorax
where do the parietal and viseceral pleura fuse?
@ the hilum
how do boyles and pouiselles law impact how pressure and flow changes in lungs?
pressure change
- Boyle’s Law: If the volume of a gas is made to increase the pressure exerted by the gas decreases
- SO, as alveoli expand: the pressure inside them decreases and gas flows in from the conducting airways. The pressure change is inversely proportional to the volume change
flow change:
- Poiseuille’s law: as the diameter increases, the flow of gas into the alveoli increases (as the fourth power of the radius of the alveolar ducts and respiratory bronchioles)
-
what is pressure change, & therfore work, like of inspiration and expiration?
(work is change in pressure times change in volume
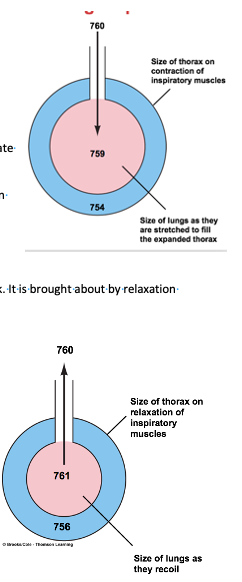
Inspiration
- increase in the size of the lungs makes the intra-alveolar pressure fall (Boyle’s Law).
- the decrease in alveolar pressure during inspiration = 1mmHg.
The small pressure difference means that the lungs are highly efficient and only a small amount of work needs to be done to inflate them
Expiration
- Expiration is a normally a passive process involving no muscle work. It is brought about by relaxation of inspiratory muscles
- The chest wall and stretched lungs recoil to their pre-inspiratory size because of their elastic properties
- The recoil of the lungs makes the intra-alveolar pressure rise above atmospheric, but again, only by 1 mm Hg.
- The air then leaves the lungs down its pressure gradient until the intra-alveolar pressure become equal to atmospheric pressure
what are two factors that cause lungs to recoil? (2) explain one
- *- elastic connective tissue in the lungs**
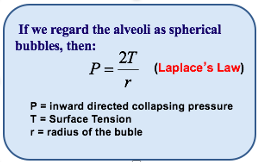
- alveolar surface tension: alveolar surface tension is the attraction between water molecules at the water-air interface. In the alveoli, this produces a force which tends to make them collapse. If the alveoli were lined with water alone the surface tension would make the alveoli completely collapse during expiration as they have no connective tissue to hold them open.
due to leplaces law - what sizee of alveoli are more likely to collase during expiration?
why is it hard to reinflate lungs after they’ve collapsed?
- due to le places law: the smaller alveoli (with smaller radius) naturally will have a higher tendency to collapse during expiration.
- collapsed alveoli are very hard to reinflate as the walls tend to stick together.
what is surfactant - explain how it works :)
which cells make it?
Pulmonary surfactant: complex mixture of lipid and protein, secreted by the type II pneumocytes (alveolar cells)
function: lowers alveolar surface tension by interspersing between the water molecules lining the alveoli. = prevents the smaller alveoli from collapsing and emptying their air contents into the larger alveoli.
With surfactant alveoli shrink evenly during expiration
what is the differnece in alveoli, during expiration, for alveoli with and without surfactant?
without surfacntant:
- During expiration:
a) smaller alveoli collapse completely
b) larger alveoli change little
with surfactant:
During expiration:
a) both alveoli decrease proportionately in size: surfactant enables you to have lungs with different sizes of alveoli in them that don’t collapse with expiration
what are the 4 different types of surfactant?
what are their different properties?
four different lipoproteins: (type A, B, C, D) which make different forms of surfactant with different properties:
- Surfactant containing lipoproteins B &C (the ‘classic’ form): reduces surface tension and ensure proper lung function.
- Surfactants containing lipoproteins A & D: coat bacteria and viruses and help the immune system deal with them. (surfactant D deficiency is a particular risk factor for pulmonary tuberculosis)
what is respiratory distress syndrome of new born?
- Foetal lungs are unable to synthesize surfactant until late in pregnancy.
- Premature babies (before ~28 weeks) may not have enough pulmonary surfactant, so the baby has to make very strenuous inspiratory efforts in an attempt to overcome the high surface tension and inflate the lungs
what is spirometry use to test? (6)
- Assess the progress and prognosis of respiratory disease in a patient.
- Assess whether lung disease is present at an early stage, i.e. prior to overt clinical disease.
- Assist in quantifying the severity of airway disease.
- Assess the effect of therapy, such as corticosteroids, bronchodilators
- Delineate risk factors, e.g. the odds of developing future respiratory disease, or operative risks.
- Monitor whether the pattern of lung growth or aging is normal.
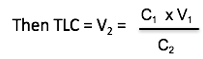
How do you measure total lung capacity (TLC?)
- inspiration of a fixed volume of a gas mixture which includes helium, followed by rebreathing the mixture until the helium is evenly distributed in the lung gases.
- Helium does not get absorbed into the blood, so if we sample the rebreathed gas it will contain a lower concentration of helium than the original inspired gas as it has penetrated the residual volume
- Let C1 be concentration of helium in inspired gas & V1 volume of inspired gas. Similarly, let C2 be concentration in rebreathed gas and V2 the volume (i.e. V2 = TLC)
what does peak flow measurement assess?
how do u test?
- peak flow rate: assesses airway resistance. The test is useful in patients with obstructive lung disease (e.g. asthma and COPD)
- how:
a) **patient taking a full inspiration
b) ** then giving a short sharp blow into the peak flow meter
c) and the average of three attempts is usually taken
what does peak flow measure change with? (2)
The peak flow rate in normal adults vary with age and height
how do u test for ventilation/perfusion (V/Q) matching?
what does reduced ventilation and normal perfusion in pneumonia cause?
what does reduced perfusion with normal ventilation in pulmonary emboli cause?
(much harder and will have to be done in specialised lung function clinics)
- Analyse with isotope scanning
- Reduced ventilation and normal perfusion in pneumonia causes hypoxaemia
- Reduced perfusion with normal ventilation in pulmonary emboli also causes hypoxaemia
- In COPD Regional V/Q mismatch reduces the efficiency of gas transfer.
explain how do you measure the efficiency of oxygen transport across the alveolar membrane?
efficiency of oxygen transport across the alveolar membrane: measured by comparing alveolar oxygen levels (PAO2) with **arterial levels (PaO2)
- alveolar oxygen partial pressure**
can be obtained by analysis with an oxygen meter of the ‘end tidal ‘expired gas, i.e. the last portion of expired gas, which will have the same composition as alveolar gas - arterial oxygen partial pressure can be measured with a pulse oximeter which measures the saturation of the haemoglobin with oxygen. The haemoglobin oxygen saturation is related to the oxygen partial pressure by the oxygen-haemoglobin saturation curve
what is exercise testing?
- How far can the patient walk, is it enough to carry out essential tasks?
- Physiotherapy and OT assessment
- Assess breathlessness on exercise with visual analogue score
- Treadmill or bicycle exercise tests show ventilation as a function of work and anaerobic threshold, which correlates with cardiopulmonary capacity and operative risk
what idoes chronic lung disease (like COPD) do to ventilation / perfusion? why
Chronic lung disease: reduces compliance of airways; this particularly affects the gas exchange at the base of the lungs as it reduces airflow into alveoli at the base of the lungs and thus reduces V/Q ratio
-
The Mediastinum27
-
CR Anatomy: Question Bank17
-
The Heart and Coronary Arteries34
-
Clinical Skills: CV1
-
The Conducting System of the Heart & ECG43
-
Anatomy: Practical 1 - Mediastinum43
-
Smooth and Cardiac Muscle32
-
CVS Histology48
-
Anatomy: Practical 2 - Thorax and the Lungs41
-
Heart as a Pump40
-
Haemodynamics35
-
Carriage of Oxygen in the Blood24
-
Review of the Sympathetic Nervous System34
-
Neural Control of Blood Pressure28
-
Renal Function 128
-
Renal Function 227
-
Blood volume & pressure control after Haemorrhage0
-
Microcirculation & Oedema35
-
Microanatomy - Histology of Hematopoietic System29
-
Peripheral Vasculature of the Limbs39
-
Drug Treatments for CVD24
-
Anatomy of the respiratory system27
-
Hormonal Control of BP32
-
Introduction to Respiratory System29
-
Anatomy of the upper airway41
-
Anatomy: Practical 2 - Thorax and the Lungs (Part 2)36
-
Pulmonary Circulation25
-
Chest X-rays28
-
Respiratory Physiology I17
-
Respiratory Physiology II25
-
:)51
-
Histology of Resp. System34
-
Pharmacology of the Airways14
-
Histology Qs7
-
Acid-Base Control of Respiration28
-
Gas Exchange and Lung Function Tests27
-
big boys29
-
::)53
-
:O50
-
:L54
-
:D13
