what is cardiac output?
what happens if different cardiac outputs occur in the ventricles?
cardiac output: Cardiac output (CO) is the amount of blood pumped by the heart minute and is the mechanism whereby blood flows around the body, especially providing blood flow to the brain and other vital organs
different cardiac outputs: blood will gradually accumulate in a ventricle and be removed by the other
Mean arterial pressure (MAP) is the product of ? and ?
Mean arterial pressure (MAP) is the product of cardiac output (CO) and total peripheral resistance (TPR):
MAP = CO × TPR
what is the difference between BP in systemic and pulmonary circulation? why?
what does this mean as a consequence for anatomy? (2)
what controls the level of blood flow to an organ?
- BP in systemic circulation high to give efficient distribution of blood to different organs
- needs thick, muscular arteries: prevents aneurisms
- needs thicker ventricles
- blood flow to organs is normally determined by state of constriction of muscles around the small arteries feeding that orgran
why is pulmonary artery pressure lower than systermic artery pressure?
total vascular resistance in the pulmonary vascular bed is much lower than in systemic circulation (so lower pressure is needed)
there is no need for high pressure because only the lungs are involved
what is BP (systolic and diastolic) of systemic and pulmonary circ in:
a) normal / starts?
b) arterioles?
c) capillaries?
d) right atrium
a) normal: 120/80 mmHg
b) arterioles: 30 mmHg
c) capillaries: 10mmHg
d) right atrium: 2mm Hg
normally: 120/80 mm Hg
- *pulmonary circ:**
a) normal: 25/8 mmHg
b) capillaries: 8-12 mmHg
d) left atrium: 5 mm Hg
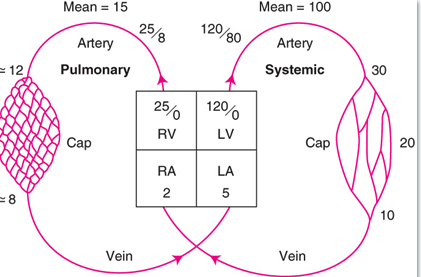
normal BP in the lungs is X mmHg or about Y of rest of bodies BP?
Normal blood pressure in the lungs is 15 -25 mmHg, or about 1/5th the bodies blood pressure.
what is starlings law of the heart?
what is the limit to starlings law? what does this result in?
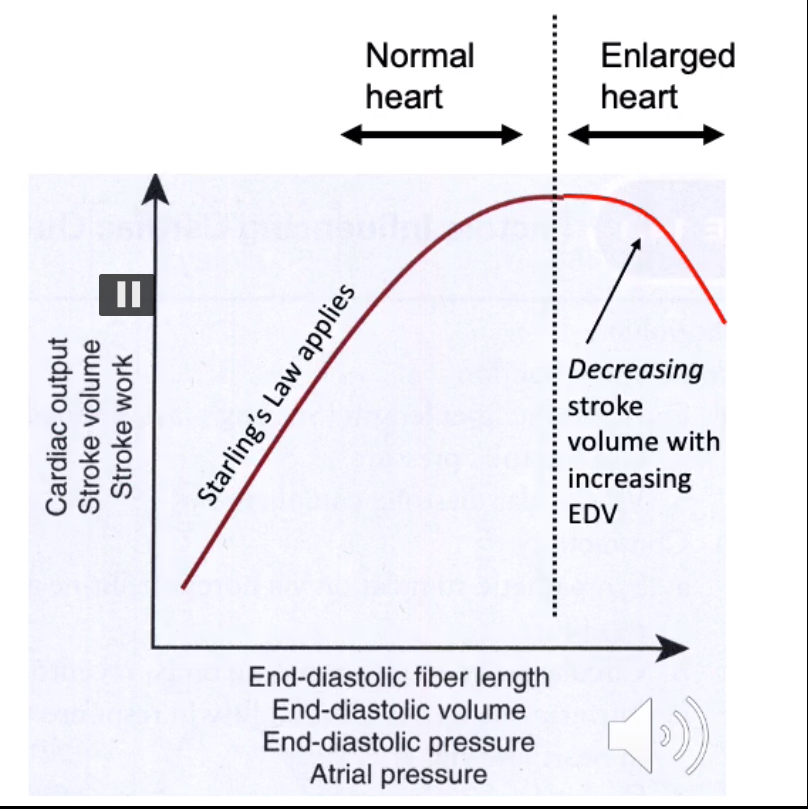
- ventricular contractile force is proproportional to end diastolic volume (aka ventricle will pump out however much blood is delivered to it by atria - more blood: more strongly pumped)
- if more blood is delivered: ventricle expands to a greater diameter & contracts more strongly
limit to starlings law:
- If the preload is too great and the ventricle expands beyond a certain volume, the mechanism fails: ventricle contracts more weakly
- this is a tipping point: beyong which heart failure starts to occur
what is preload?
what is preload directly proportional to?
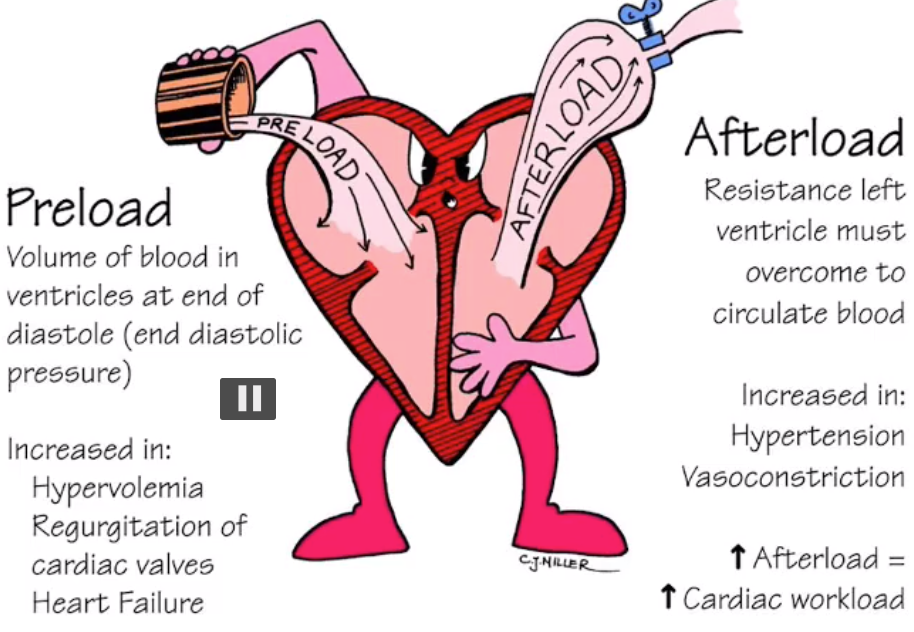
- *pre-load:
- **volume of blood at end of diastolic filling - stretch
- the difference between end diastolic and systolic volumes called: preload. determined by the volume of blood delivered to heart by IVC and SVC
(another way of looking at preload is: the degree of stretching experienced by the ventricle during diastole is called the preload)
preload determines X of the ventricles?
what does this ^ in turn determine in the heart?
- preload determines the end diastolic volume (EDV) of the ventricles
- in turn, determins the stroke volume: (the volume of blood pumped out heart per beat)
what is stroke volume? what is it normally in healthy human?
what is end-diastolic volume? how does it differ to stroke volume?
what is residual volume? what is normally in healthy
stroke volume: the volume of blood pumped out of heart per beat - usually 70ml
end diastolic volume: the amount of blood that is in the ventricles before the heart contracts.
differ because: there is always some blood left in the ventricle at end of systole: residual volume (ESV)
what is EDV and ESV?
what is EDV and ESV values in healthy heart?
ventricular end-diastolic volume (EDV) and the end-systolic volume (ESV).
The EDV is the filled volume of the ventricle prior to contraction
ESV is the residual volume of blood remaining in the ventricle after ejection.
EDV: 120 ml
ESV: 50 ml
(120 - 50 = 70 ml = stroke volume!)
how do u calculate stroke volume?
EDV-ESV
why is an enlarged heart a bad sign?
what does larger end diastolic volume produce ^?
- enlarged heart = enlarged ventricles
- enlarged ventricles will not have corresponding increase in ventricular wall thickness, so will contract more weakly than a smaller heart
- this is bc the heart fibres are stretched to point where Starling mechanism no longer works
larger end diastolic volume produces a smaller stroke volume: heart failure
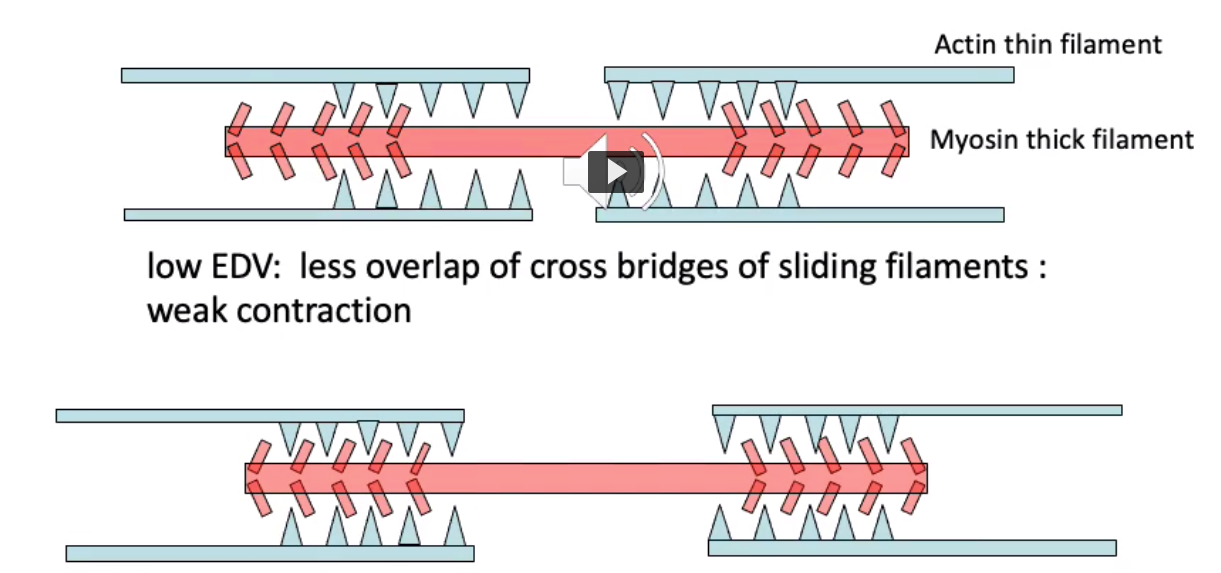
what is the mechanism underlying starlings law?
at low EDV: there is less overlap of cross bridges (of actin and myosin): weak contraction
at high EDV: more overlap of cross bridges stronger contraction
increasing the overlap of active region of A & M increases the force of contraction
what is afterload?
what does afterload depend on ? (2)
This is the effective flow impedance (dyanmic resistance) of the aorta and large arteries (resistance left ventricle must overcome to circulate the blood)
Afterload depends on the diameter & elasticity of the tissue
what is the reciprocal of impedence?
what does a higher ^ of aorta do to afterflow?
compliance
higher compliance of aorta = lower afterload = less work the heart has to do for cardiac output
what effect does altering afterload have on the cardiac workload?
increasing afterload = increasing cardiac workload
what is inotropy?
which factors increase inotropy?(7)
inotropy: the contractility (force of contraction) of the ventricular muscle
factors that increase inotropy:
Increased blood calcium levels
Beta adrenergic agonists (such as adrenaline - increases contractility)
Excess thyroid hormone
Drugs which stimulate calcium entry into the myocardium, e.g. levosimendan
Cardiac glycosides (e.g. digoxin)
Insulin (increases inotropy)
Glucagon
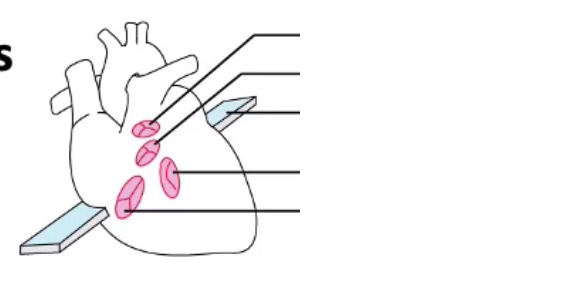
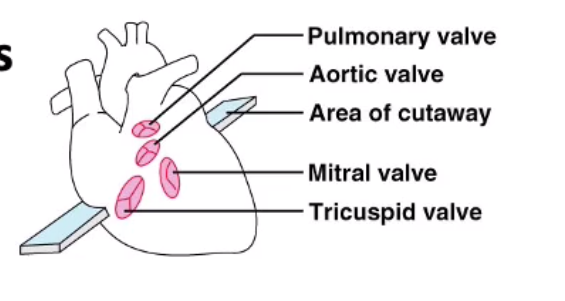
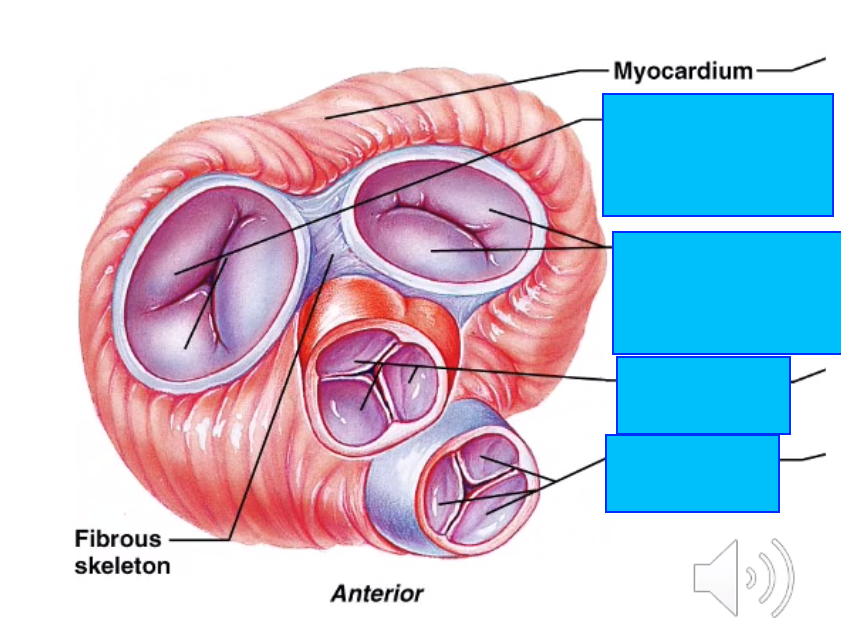
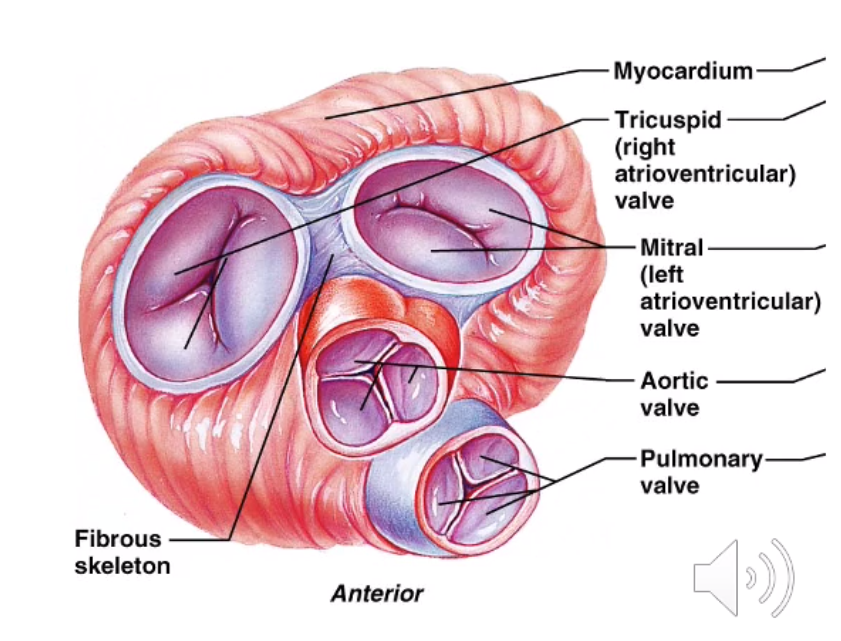
the atrioventricular valves are controlled by which muscles?
the atrioventricular valves are kept in position by what?
AV valves are controlled by papillary muscles
AV valves are kept in positon by chordiane tedinae
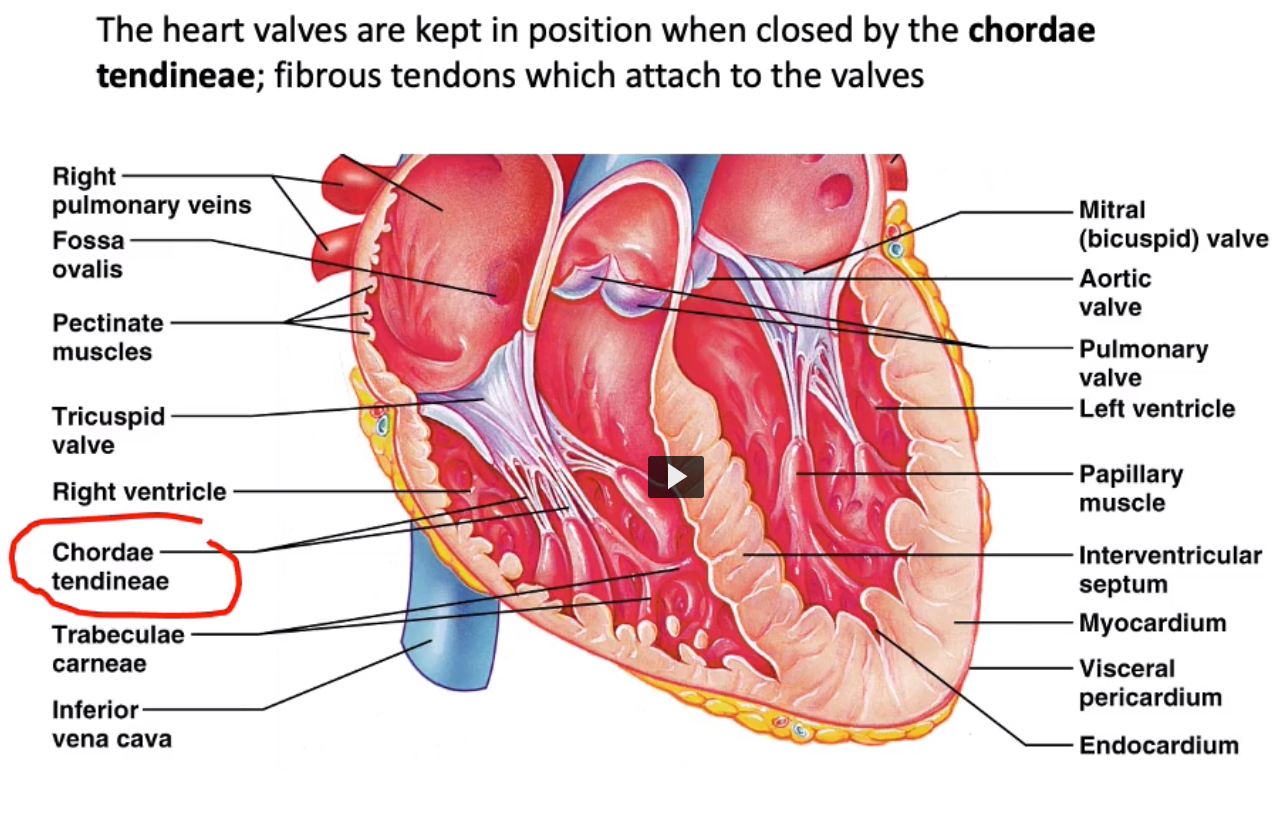
Right atrio-ventricular valve is the X (due to the X valve leaflets)
Left atrio-ventricular valve is the X valve (or X valve, has X valve leaflets)
Right atrio-ventricular valve is the tricuspid valve (due to the 3 valve leaflets)
Left atrio-ventricular valve is the mitral valve (or bicuspid valve, has 2 valve leaflets)
which are first muscles to contract during systole?
what does this cause to happen?
- papillary muscles contract first during systole
- pull on the chordinae tendianeae and pull the valves closed
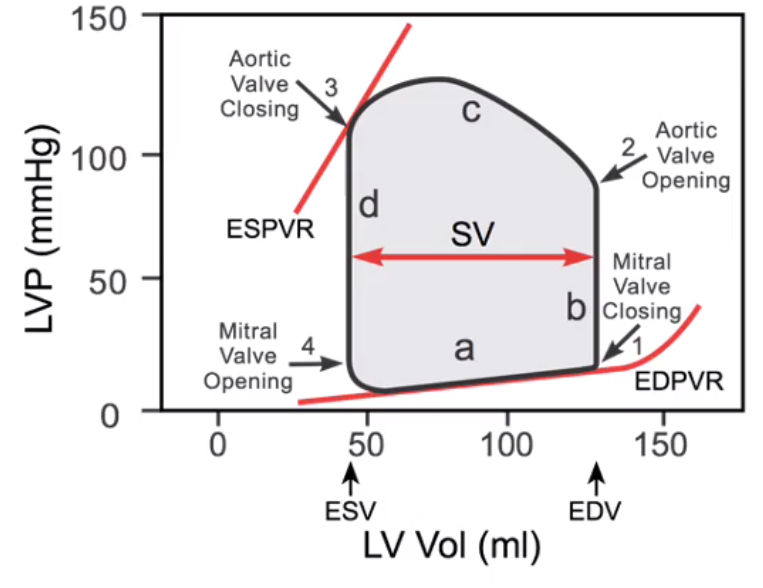
explain the pressure profiles in the left atrium, left ventricle and the aorta for a single cardiac cycle, using the diagram below
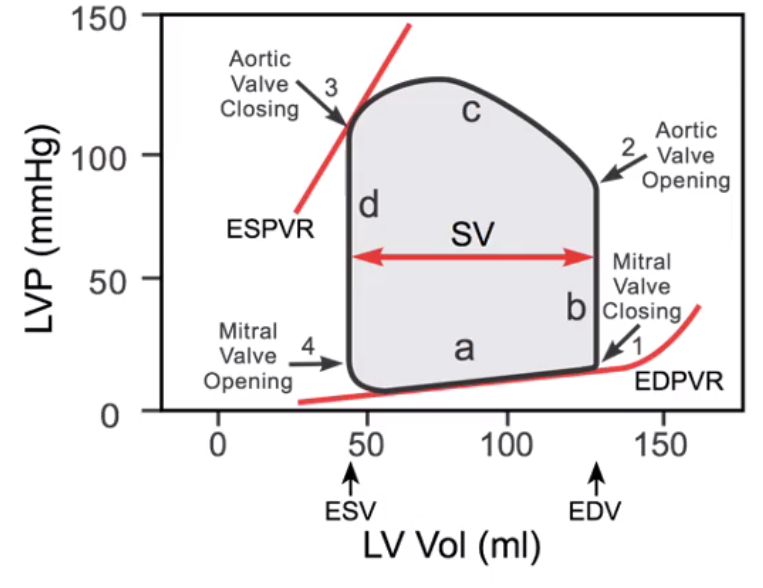
- start at the point marked ’mitral valve opening’. The left ventricle is at its minimum volume having just completed systole
- As the ventricle fills we travel up the lower slope ‘a’ from ESV (end systolic volume) to EDV (end diastolic volume).
- The ventricle starts to contract and the pressure rises steeply along the vertical line ‘b’.
- At point ‘1’ the mitral valve closes as the ventricle has started to contract.
- Initially the ventricular pressure rises due to ventricular contraction but the volume stays constant as the aortic valve is closed. This the isovolumentric contraction phase, hence line ‘b’ is vertical.
- When the pressure in the ventricle is greater than that in the aorta the aortic valve opens (point 2)
- Now the ventricular volume decreases as it ejects blood into the aorta; note the humped appearance of the curve ‘c’.
- At some point beyond ‘c’ the ventricle stops contracting; now the pressure drops until it is below that in the aorta and the aortic valve closes (point ‘3’). The pressure in the ventricle drops rapidly at a constant end systolic volume (ESV).
- Eventually we return to point ‘4’ where the ventricular pressure drops below that in the atria, the mmitral valve opens and the cycle repeats.












-
The Mediastinum27
-
CR Anatomy: Question Bank17
-
The Heart and Coronary Arteries34
-
Clinical Skills: CV1
-
The Conducting System of the Heart & ECG43
-
Anatomy: Practical 1 - Mediastinum43
-
Smooth and Cardiac Muscle32
-
CVS Histology48
-
Anatomy: Practical 2 - Thorax and the Lungs41
-
Heart as a Pump40
-
Haemodynamics35
-
Carriage of Oxygen in the Blood24
-
Review of the Sympathetic Nervous System34
-
Neural Control of Blood Pressure28
-
Renal Function 128
-
Renal Function 227
-
Blood volume & pressure control after Haemorrhage0
-
Microcirculation & Oedema35
-
Microanatomy - Histology of Hematopoietic System29
-
Peripheral Vasculature of the Limbs39
-
Drug Treatments for CVD24
-
Anatomy of the respiratory system27
-
Hormonal Control of BP32
-
Introduction to Respiratory System29
-
Anatomy of the upper airway41
-
Anatomy: Practical 2 - Thorax and the Lungs (Part 2)36
-
Pulmonary Circulation25
-
Chest X-rays28
-
Respiratory Physiology I17
-
Respiratory Physiology II25
-
:)51
-
Histology of Resp. System34
-
Pharmacology of the Airways14
-
Histology Qs7
-
Acid-Base Control of Respiration28
-
Gas Exchange and Lung Function Tests27
-
big boys29
-
::)53
-
:O50
-
:L54
-
:D13
