Facial nerve:
what type of innervation?
what is the course of the facial nerve?
what type of innervation?
sensory, motor and parasympathetic
what is the course of the facial nerve?
Once the facial nerve has passed through the internal acoustic meatus it enters the facial canal, and this is where the geniculate ganglion is found.
Lastly, the facial nerve gives off the following branches before exiting the cranium via the stylomastoid foramen:
- Greater petrosal nerve, which is parasympathetic fibres to the mucous glands and lacrimal glands
- Nerve to stapedius, a muscle of the middle ear
- Chorda tympani, special sensory fibres to anterior 2/3rds of the tongue, as well as parasympathetic fibres to the submandibular and sublingual glands
This facial nerve now exits the stylomastoid foramen, which is a small foramen in-between the styloid process and the mastoid process of the temporal bone.
After exiting the skull, the first branch is the posterior auricular nerve which provides some motor innervation to the muscles around the ear.
Immediately distal to this, motor branches are sent to the posterior belly of the digastric muscle and to the stylohyoid muscle (suprahyoid muscles).
The main trunk of the nerve continues anteriorly and inferiorly to the parotid gland, YET DOESN’T INNERVATE IT. INNERVATION TO THE PAROTID GLAND IS VIA THE GLOSSOPHARYNGEAL NERVE. Within the parotid gland, the facial nerve now terminates by splitting into its 5 branches:
- Temporal branch
- Zygomatic Branch
- Buccal branch
- Marginal mandibular branch
- Cervical branch
what is the geniculate ganglion?
where does it send innervation to
a collection of pseudounipolar sensory neurons of the facial nerve located in the facial canal of the head.
This is a collection of fibres that receives motor, sensory and parasympathetic components from the facial nerve, and sends innervation to the lacrimal glands, 2 of the 3 salivary glands, tongue, palate, pharynx, facial expression muscles, etc.
This geniculate ganglion also contains the special sensory fibres from the chorda tympani nerve, a branch of the facial which supplies taste sensation to the anterior 2/3rds of the tongue.
which muscles of facial expression are innervated by
- Temporal branch [3]
- Zygomatic Branch [1]
- Buccal branch [3]
- Marginal mandibular branch [1]
- Cervical branch [1]
which muscles of facial expression are innervated by
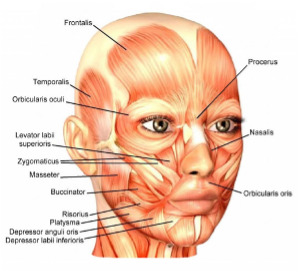
- Temporal branch: frontalis, orbicularis oculi and corrugator supericilli
- Zygomatic Branch: orbicularis oculi
- Buccal branch: orbicularis oris, buccinaot and zygomaticus muscles
- Marginal mandibular branch: mentalis muscle
- Cervical branch: plastyma
how do u do examination of CN VII?
Examination of the facial nerve
- Inspect the patients face at rest for asymmetry: do they have forehead wrinkles, nasolabial folds, angles of the mouth?
Ask the patient to perform specific facial movements:
- Raised eyebrows as if surprised: note asymmetry
- Closed eyes: scrunch up your eyes and don’t let me open them. Assess power
- Blow out the cheeks and don’t let me deflate them. Assess power
- Pursed lips: attempt to whistle
- Close lips tight and don’t let me open them
what are the parts of VN 8? [2]
vestibular fibres and cochlear fibres. Both have purely sensory function
which foramen does CN8 leave skull by? [1] describe its path and when it splits
what does CN8 innervate & what is their function [4]
distal aspect of the internal acoustic meatus, the vestibulocochlear nerve splits, forming the vestibular nerve and the cochlear nerve.
The vestibulr nerve innervates the vestibular system of the inner ear, which is responsible for detecting balance.
The cochlear nerve travels to the cochlea of the inner ear, forming the spiral ganglia which serve the sense of hearing.
how do u examine CN8?
- Ask the patient if they have noticed a change in hearing
- Assess each ear individually, standing behind the patient
- Mouth approx. 15cm from the ear, whisper a number or word and ask the patient to repeat these back to you. Cover up the ear not being tested by rubbing the tragus
- If the patient repeats these correctly, do it at arms length. Normal hearing allows whispering at 60cm
- Vestibulo-ocular reflex, which involves you turning their head quickly yet these must fixate on your nose at all times. Normally, fixation is maintained but loss of vestibular function on one side means the eyes will first move in the direction of the head, then will correct itself
what is bells palsy?
causes
symptoms
treatment
what is bells palsy?
causes
- compression of nerve
- weakness or paraylsis on one side of face
- If the protective covering of the nerve becomes damaged (i.e. epineurium) then the signals traveling from the brain to the muscles of facial expression may not be transmitted properly, leading to weakened or paralyses facial muscles
- exact reason why this happens is not clear: it may be due to a virus (herpes usually causes inflammation of CN VII), or possibly chickenpox, shingles, EBC, mumps, influenza B, etc).
symptoms
- loss of contraction of muscles of facial expression
- eye will droop, as orbicularis oculi no longer innervated
- drooping corner of mouth due to loss of innervation of orbicularis oris
- no muscle tone so cannot puff your cheeks
treament
- Most people recover from Bell’s palsy in 1-2 months
- Treating with a hormone called prednisolone can speed up recovery
- Eye lubrication will be needed, as the patient is not blinking properly due to loss of innervation of orbicularis oculi and levator palpebrae superioris. Therefore, the eye will be exposed and tears which usually lubricate the eye will be evaporated. Therefore, artificial tears can be supplied in the form of teardrops to keep the eye lubricated
- Those who cannot shut their eye properly will also need to be supplied with surgical tape to keep their eye shut. The man in the PBL scenario needed both eyedrops and this tape in order to keep his eyes intact
- steriods: reduce inflammation and allow the nerve to decompress
How does Bell’s palsy differ from a stroke?
- Facial nerve palsy = LMN deficit affecting facial nerve (all motor branches)
- Known as Bell’s Palsy - cause unknown (idiopathic). Sometimes think it could be viral infection, or general inflammation, but generally idiopathic. Very hard to treat.
- Results in paralysis of whole ipsilateral side of face
This is a different presentation to a stroke
- Stroke = UMN deficit within cerebral cortex
- There is bilateral UMN innervation to the upper face
- If UMN in one side of the brain are damaged (stroke) there is some compensation to the upper face from the other side of the cortex
- So when a stroke occurs, there will be paralysis on the OPPOSITE side (due to contralateral deficit in UMN) yet the forehead will not be changed as the UMN are ‘shared in the forehead’ rather than being separate on both sides.
- Paralysis of lower half of contralateral face
is bells palsy a LMN or UMN condition? [1]
is bells palsy a LMN or UMN condition? [1]
LMN
stroke:
two types? [2]
Stroke is defined as an acute neurological deficit lasting more than 24 hours and caused by cerebrovascular aetiology.
It is subdivided into ischaemic stroke (caused by vascular occlusion or stenosis) and haemorrhagic stroke (caused by vascular rupture, resulting in intra-parenchymal and/or subarachnoid haemorrhage).
what is TIA?
A transient ischaemic attack (TIA) or “mini stroke” is caused by a temporary disruption in the blood supply to part of the brain.
The disruption in blood supply results in a lack of oxygen to the brain.
This can cause sudden symptoms similar to a stroke, such as speech and visual disturbance, and numbness or weakness in the face, arms and legs.
But a TIA does not last as long as a stroke. The effects last a few minutes to a few hours and fully resolve within 24 hours.
what are symptoms of stroke? [5]
Sudden numbness or weakness in the face, arm, or leg, especially on one side of the body.
Sudden confusion, trouble speaking, or difficulty understanding speech.
Sudden trouble seeing in one or both eyes.
Sudden trouble walking, dizziness, loss of balance, or lack of coordination.
Sudden severe headache with no known cause.
the 4 main stroke symtpoms can be remembered using … what?
FAST
Face – the face may have dropped on 1 side, the person may not be able to smile, or their mouth or eye may have drooped.
Arms – the person may not be able to lift both arms and keep them there because of weakness or numbness in 1 arm.
Speech – their speech may be slurred or garbled, or the person may not be able to talk at all despite appearing to be awake; they may also have problems understanding what you’re saying to them.
Time – it’s time to dial 999 immediately if you notice any of these signs or symptoms.
what are the causes of ischaemic & haemorrhagic stroke?
ischaemic stroke:
happens when the brain’s blood vessels become narrowed or blocked, causing severely reduced blood flow (ischemia). Blocked or narrowed blood vessels are caused by fatty deposits that build up in blood vessels or by blood clots or other debris that travel through the bloodstream, most often from the heart, and lodge in the blood vessels in the brain
Hemorrhagic stroke
Hemorrhagic stroke occurs when a blood vessel in the brain leaks or ruptures. Brain hemorrhages can result from many conditions that affect the blood vessels. Factors related to hemorrhagic stroke include:
- Uncontrolled high blood pressure
- Overtreatment with blood thinners (anticoagulants)
- Bulges at weak spots in your blood vessel walls (aneurysms)
- Trauma (such as a car accident)
- Protein deposits in blood vessel walls that lead to weakness in the vessel wall (cerebral amyloid angiopathy)
- Ischemic stroke leading to hemorrhage
risk factors for ischaemic stroke? [4]
risk factors for H stroke? [4]
risk factors for ischaemic stroke? [4]
- things that increase chances of atherosclerosis:
smoking
high blood pressure (hypertension)
obesity
high cholesterol levels
diabetes
excessive alcohol intake
atrial fibrillation
risk factors for H stroke? [4]
main cause = high BP
- Things that increase the risk of high blood pressure include:
being overweight
drinking excessive amounts of alcohol
smoking
a lack of exercise
stress
non modifiable risk factors for stroke?
non modifiable risk factors for stroke?
age – you’re more likely to have a stroke if you’re over 55, although about 1 in 4 strokes happen to younger people
family history – if a close relative (parent, grandparent, brother or sister) has had a stroke, your risk is likely to be higher
ethnicity – if you’re south Asian, African or Caribbean, your risk of stroke is higher, partly because rates of diabetes and high blood pressure are higher in these groups
your medical history - previous history of stroke
what is atrial fibrillation?
Atrial fibrillation refers to irregular atrial contraction, caused by chaotic impulses.
what are causes of atrial fibrillation
unsynchronised contractions of the atria
It is defined as a supraventricular arrhythmia because the abnormality originates above the ventricles in the atria. Classically, there are multiple waves of electrical activity leading to fragmentation of the normal coordinated electrical activity within the atria. This causes the cardiomyocytes to contract independently leading to ‘fibrillation’.
what are the hallmark ECG features of atrial fibrillation? [3]
AF is characterised by the presence of an irregularly irregular pulse on examination. This is confirmed on a 12-lead ECG or appropriate ECG monitoring. The hallmark ECG features of AF include:
Irregularly irregular rhythm
Absence of P waves (no coordinated atrial activity)
Irregular, fibrillating baseline.
what are 3 types of AF? [3]
Paroxysmal: recurrent episodes (≥30 seconds in duration) that terminate spontaneously or with intervention within 7 days
Persistent: AF that fails to self-terminate within 7 days. If lasts >12 months known as ‘long-standing persistent AF’
Permanent: a term used to describes patients where sinus rhythm cannot be restored or maintained and AF is the accepted final rhythm
what are cardiac and non cardiac causes of AF?
Cardiac
Hypertension
Ischaemic heart disease
Valvular disease (e.g. rheumatic heart disease)
Myocardial infarction
Cardiomyopathy
- *Non-cardiac**
- *Respiratory**: COPD, pneumonia, pulmonary emoblism
- *Endocrine**: hyperthyroidism, diabetes mellitus
- *Acute infection**
- *Electrolyte disturbances**: hypokalaemia, hypomagnesaemia, hyponatraemia
- *Drugs**: bronchodilators, thyroxine
- *Lifestyle factors:** alcohol, excessive caffeine, obesity
what is going on electrophysiologically with AF?
In AF, there is disruption of the normal electrophysiological mechanisms in the atrial myocardium.
Instead of coordinated electrical activity from the sinoatrial node (SAN) across the atria, there are fragmented impulses generated all over the atria. Different mechanisms have been proposed with varying degrees of evidence to support their existence.
what are signs and symptoms of AF?
Symptoms
Asymptomatic
Palpitations
Shortness of breath
Angina
Presyncope
Lethargy
Signs
Irregularly irregular pulse
Absent ‘a’ wave on JVP: corresponds to atrial contraction
Tachycardia
Hypotension
Features of heart failure: bibasal crackles, raised JVP, peripheral oedema
-
FunMed Week 225
-
FunMed Week 3: SCA29
-
FunMed Week 4: Breast30
-
FunMed Week 5: Infection33
-
FunMed Week 6: AD23
-
FunMed Week 710
-
FunMed Week 8: Vaccination22
-
CR Week 126
-
CR Week 223
-
CR Week 324
-
Met121
-
Met222
-
Met329
-
Loco112
-
Loco25
-
Loco312
-
BB17
-
BB226
-
BB339
-
HD126
-
HD1b22
-
HD 225
-
HD 319
-
Seen PBL155
-
Seen PBL247
-
MET :O14
