Q1: Explain how inhalation of allergens may lead to shortness of breath in patients with asthma? (3 marks)
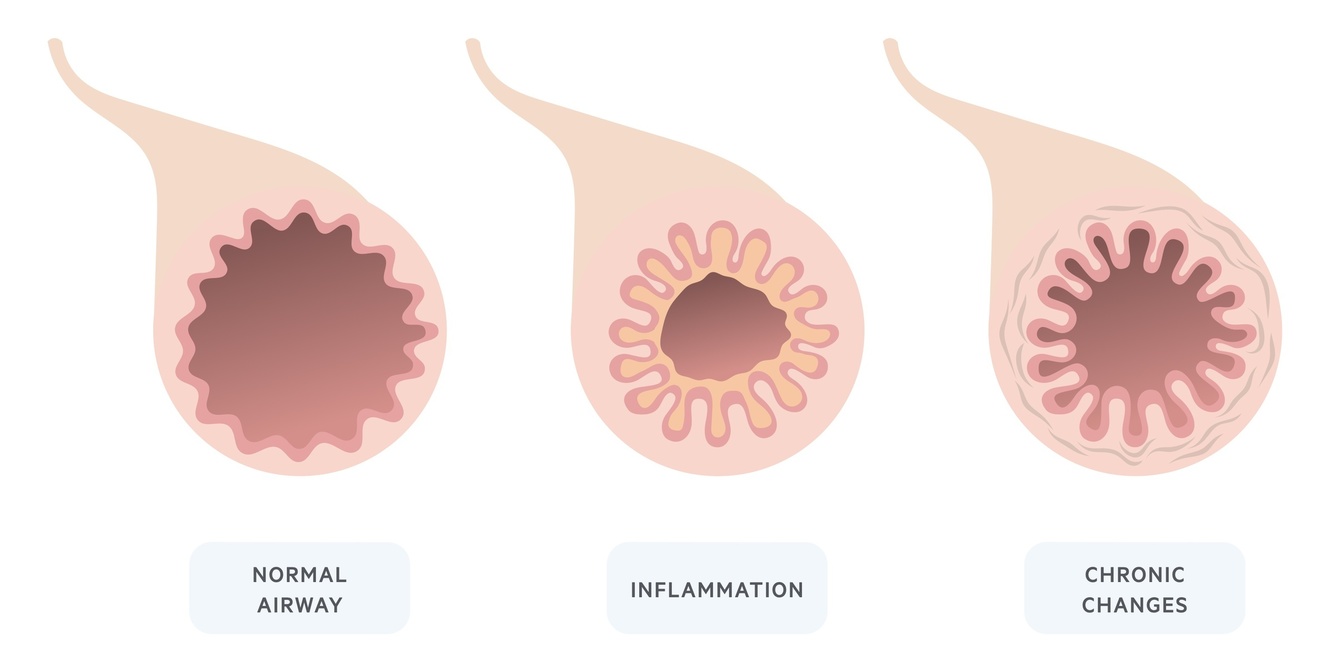
Allergens in the airways may cause airway inflammation (1 mark),
which may lead to airway narrowing (1 mark).
Narrowing of the airways will lead to reduced airflow (1 mark) and consequently shortness of breath.
Q2: Explain what a peak flow device measures. (2 marks)
A peak flow devise measures peak expiratory flow, the maximal flow of air (1 mark) during forced exhalation (1 mark).
Q3: Explain why patients with asthma may have a normal PEF? (2 marks)
Patients with well-controlled asthma (1 mark) may have normal PEF, as airflow limitation in asthma is variable (reversible) (1 mark).
Q4: Describe the role and mechanism of action of inhaled corticosteroids? (3 marks)
Inhaled corticosteroids (ICS) are used as preventer/maintenance therapy (1/2 mark) in asthma to reduce airway inflammation (1/2 mark)
ICS reduce airway inflammation by dampening gene expression of pro-inflammatory mediators (1 mark*) via the glucocorticoid receptor (GR) (1 mark)
*will accept the following: increase expression of anti-inflammatory genes
what is the difference in response to allergen in normal and healthy person?
- Normal:
- A low level T-helper (TH-2) response. This produces an IgG response
- Asthma:
- allergen digested by antigen presenting cellsdigested and presented by MHC Class II molecules
- CD4 cells activate the TH-2 lymphocytes through the release of IL4, IL5, IL13.
- The activated TH2 cells release cytokines (IL4) which recruit multiple inflammatory cells, NK cells eosinophils, mast cells, and IgE producing Cells causes the release of histamines
- IgE mediated mechanism: (IgE: antibody associated with allergic response)
- binding of an allergen to IgE-mast cells results in their rapid degranulation and the release of inflammatory compounds, including histamine, which contribute to local inflammation and the symptoms associated with allergy.
- The activated TH2 cells release cytokines (IL4) which recruit multiple inflammatory cells, NK cells eosinophils, mast cells, and IgE producing Cells causes the release of histamines
explain the difference between sensitisation and provacation of an allergy?
In type I HS sensitization, allergen triggers production of allergen-specific IgE that binds via its Fc region to mast cell and basophil FcεRs.
In the early effector stage, re-exposure of sensitized mast cells to allergen triggers immediate degranulation and release of pre-formed mediators, and synthesis of inflammatory molecules
what are the 3 causes of airflow limitation in asthma? [3]
Bronchoconstriction
Airway oedema
Airway remodelling
explain mechanism of bronchoconstriction occuring in asthma patients
- Ach binds to M3 receptor
- causes IP3 to be released
- IP3 binds to IP3 Receptor - IP3R on ER
- causes Ca2+ released into cytoplasm
- increase in intracellular Ca2+ binds to calmodulin & myosin light chain kinase (MCLK)
- phosphorylases light chain on myosin
- - actin-myosin cross link occurs & SMC occurs
in simple terms, what is bronchoconstriction caused by/
- In acute exacerbations of asthma, bronchial smooth muscle contraction (bronchoconstriction) occurs quickly to narrow the airways in response to exposure to a variety of stimuli including allergens or irritants. Allergen-induced acute bronchoconstriction results from an IgE-dependent release of mediators from mast cells that includes histamine, tryptase, leukotrienes, and prostaglandins that directly contract airway smooth muscle
what causes airway oedema in asthma patients
- As the disease becomes more persistent and inflammation more progressive, other factors further limit airflow. These include oedema, inflammation, mucus hypersecretion and the formation of inspissated mucus plugs, as well as structural changes including hypertrophy and hyperplasia of the airway smooth muscle. These latter changes may not respond to usual treatment.
what are risk factors for asthma?
- Family history: Multiple genes are implicated that predispose people to hyper-responsiveness to environmental aetiological triggers.
- Allergens:
- cats, dogs, cockroaches, dust mites, fungal spores, tobacco smoke, fumes from chemicals (e.g., bleach), and pollen from trees, weeds, and grass.
- Workers commonly affected by occupational allergens include bakers, farmers, carpenters, and people involved in manufacturing plastics, foams, and glues.
- Atopic history: History of eczema, atopic dermatitis, allergic rhinitis is strongly associated.
what are Immunohistopathologic features of asthma? [5]
- Neutrophils (especially in sudden-onset, fatal asthma exacerbations; occupational asthma, and patients who smoke)
- Eosinophils
- Lymphocytes
- Mast cell activation
- Epithelial cell injury
what are signs of asthma? [4]
- Wheezing on auscultation
- Intercostal recession in children
- Severe attacks render people unable to speak
- Prolonged expiratory phase (respiratory and expiratory phases should be equal)
how do u treat asthma?
- Reliever inhalers: bronchodilators – blue inhaler
- SABAs
- Salbutamol
- Terbutaline
- SABAs
- Preventer inhalers:
- low dose inhaled cortical steroids (ICS) (anti-inflamm drugs) - take for rest of life
- Beclomethasone diproprionate – brown inhaler
- Budesonide
- Ciclesonide
- Fluticasone propionate
- LABAs
- low dose inhaled cortical steroids (ICS) (anti-inflamm drugs) - take for rest of life
- SAMA and LAMAs for severe asthma only
what is mechanism of SAMA & LAMA
and
SABA & LABA?
- Mechanism of inhalers:
- Airway smooth muscle cells have both M3 muscarinic receptors & beta2 adrenergic receptors
- SAMA & LAMA: block the binding of ACh to M3 muscarinic receptors - bring about smooth muscle relaxation
- SABA & LABA: activate beta2-adrenergic receptors - induce cascade of signalling events = smooth muscle relaxation
what is mechansim of ICS in lungs for asthma?
- Mechanism of action of inhaled cortical steroids in lungs:
- cortical steroid crosses cytoplasm & binds to glucocorticoid receptor - activates into glucocorticoid response element (GRE)
- GRE binds to nucleus:
- a) encodes for anti-inflam. genes
- b) recruits machinery that leads to down regulation of gene expression of pro-inflam mediators: IL-6, TNF-a & CXCL8
explain different diagnostics used for asthma?
- FEV1/FVC ratio: FEV₁/FVC <80% of predicted.
- Peak expiratory flow rate (PEFR):
- Peak flow is a measure of how quickly you can blow air out of your lungs. You measure peak flow by blowing as hard and as fast as you can into a small hand-held device called a peak flow meter.
- People get different peak flow scores depending on their age, height, and gender.
- Keep a peak flow diary : twice a day (same time each day) need to record for two weeks to get a PB. Say if you’ve had symptoms each day
- Fractional exhaled nitric oxide: (FeNo)
- breathe into a machine that measures the level of nitric oxide in your breath
- Reflective of the degree of eosinophilic inflammation
what does atopy mean?
Atopy is a genetic predisposition to IgE-mediated allergen sensitivity.
what are 4 causes of asthma [4]
atopy: Atopy is a genetic predisposition to IgE-mediated allergen sensitivity.
Aspirin-induced asthma: A small subset of patients with asthma are affected by a sensitivity to aspirin. Ingestion is capable of triggering an attack
Occupational asthma: around 15% of cases of asthma in adults are related to occupational exposure. Asthma may be induced or exacerbated by such exposure
Exercise-induced asthma: In this variant asthma is triggered by strenuous physical activity. The aetiology is complex but exposure to cold air and environmental pollutants contributes.
what happens due to chronic asthma?
Chronicity
In response to persistent chronic inflammation, the airways lay down fibrous tissue. Over time airway remodelling occurs and manifests as fixed airway obstruction - i.e. airway narrowing that is irreversible.
what are FVC and FEV1? 2]
what are FVC, FEV1 and FEV1/FVC in asthma patients? [3]
FVC: the forced (expiratory) vital capacity is a persons maximal expiration following full inspiration.
FEV1: the forced expiratory volume in one second, i.e the volume of FVC expelled after one second.
The following changes are seen in obstructive lung disease:
FVC: may be normal but often reduced due to air trapping.
FEV1: reduced.
FEV1/FVC: < 70%.
what is FeNo testing?
(what is the % in asthma patients? )
Fractional exhaled nitric oxide (FeNO)
FeNO testing is typically offered to patients being investigated for asthma at the same time as spirometry. FeNO is a newer way of testing for eosinophilic airway inflammation.
FeNO is measured in parts per billion and a level >25 ppb at 50 ml/sec is seen in 70-80% of patients with untreated asthma. Eosinophilic airway inflammation has been linked to the response to corticosteroids.
(FeNO > 40 ppb: supports a diagnosis of asthma
FeNO 25-39 ppb: suggestive of a diagnosis of asthma. Peak flow variability useful.
FeNO < 25 ppb: does not support a diagnosis of asthma)
what are the two different drug classes for treating asthma and how do they work?
Beta-receptor agonists: bind to beta receptors of the sympathetic nervous system. Causes relaxation of airway smooth muscle and subsequent bronchodilation. May be short or long-acting.
Corticosteroids: inhaled corticosteroids work by reducing inflammation within the lungs. They are thought to reduce the number of exacerbations and improve the efficacy of bronchodilators
patients with asthma also suffer from other IgE-mediated atopic conditions such as: [2]
atopic dermatitis (eczema)
allergic rhinitis (hay fever)
-
FunMed Week 225
-
FunMed Week 3: SCA29
-
FunMed Week 4: Breast30
-
FunMed Week 5: Infection33
-
FunMed Week 6: AD23
-
FunMed Week 710
-
FunMed Week 8: Vaccination22
-
CR Week 126
-
CR Week 223
-
CR Week 324
-
Met121
-
Met222
-
Met329
-
Loco112
-
Loco25
-
Loco312
-
BB17
-
BB226
-
BB339
-
HD126
-
HD1b22
-
HD 225
-
HD 319
-
Seen PBL155
-
Seen PBL247
-
MET :O14
