In women undergoing prosthetic breast reconstruction complicated by an expander/implant infection, which of the following is the most common gram-negative bacteria isolated from cultures?
A) Escherichia coli
B) Klebsiella
C) Proteus
D) Pseudomonas
E) Serratia
The correct response is Option D.
Tissue expander/implant-based breast reconstruction remains the most common form of reconstruction after mastectomy. One of the most potentially devastating complications of this form of breast reconstruction is an implant infection with need for removal of the expander/implant. The mean reported incidence of implant infection after breast reconstruction is 8%, with a range of 1 to 35%. When cultures are obtained, the most common causative bacteria on microbiology examination are gram-positive organisms (41 to 83%), specifically, Staphylococcus species (56 to 76.5%). Gram-negative bacteria accounted for 15.3 to 28.6%, with Pseudomonas (10.7 to 14%) being the most common gram-negative bacteria present on microbiology examination.
A 45-year-old woman comes to the office for consultation regarding severe breast asymmetry after undergoing lumpectomy and radiation therapy for ductal carcinoma of the right breast 5 years ago. Physical examination shows the radiated right breast is tight and retracted, and the left breast is ptotic. Left-sided mastopexy for symmetry and autologous fat grafting to the radiated breast are recommended. The patient asks if the procedure will be covered by insurance. Which of the following is the most appropriate response?
A) Fat grafting the right breast will be covered by insurance but the mastopexy will be considered cosmetic and will not be covered
B) Insurance companies rarely cover the cost of immediate breast reconstruction
C) Insurance may not cover the procedure since insurers are not mandated to pay for reconstruction of lumpectomy defects
D) Procedures for both sides will be covered by insurance
E) The left-sided mastopexy will likely be covered but the fat grafting will not be covered
The correct response is Option C.
The Women’s Health and Cancer Rights Act, signed into law in 1998, requires insurance plans to cover the cost of breast reconstruction after mastectomy. The law includes all stages of reconstruction as well as contralateral procedures to provide symmetry. An often misunderstood aspect of the Women’s Health and Cancer Rights Act is that it does not apply to individuals undergoing breast conservation therapy (lumpectomy with radiation). As rates of breast conservation therapy have continued to increase (60% of women with stage I cancers), so have significant lumpectomy defects associated with the untoward effects of radiation. In the clinical scenario presented, the patient should be informed that the corrective operation (fat grafting and mastopexy) might not be covered by her insurance company.
A 39-year-old woman is referred for consultation regarding reconstruction of the left breast two years after mastectomy for breast cancer. Implantation of a silicone prosthesis and reconstruction with a pedicled latissimus dorsi musculocutaneous flap are planned. This patient will most likely show deficits in which of the following shoulder functions?
(A) Extension and abduction
(B) Extension and adduction
(C) Flexion and abduction
(D) Flexion and adduction
(E) No deficits
The correct response is Option B.
Transfer of the latissimus dorsi musculocutaneous flap is associated with deficits in extension and adduction.
The latissimus muscle acts synergistically with six other muscles in the shoulder. The primary contribution of the muscle is in shoulder extension, adduction, and medial rotation. There are definite biomechanical changes that occur in the shoulder girdle with latissimus muscle transfer. The synergistic action of the teres major muscle compensates for loss of the latissimus muscle. This leads to teres major hypertrophy in the long term. A study in 1986 evaluated a series of patients with latissimus muscle transfer and found a decrease in total shoulder strength up to 34% compared to the contralateral side. When tested specifically for the latissimus muscle function, the average weakness was 18%. Active range of motion at the shoulder with extension and adduction was decreased by 5% and 0%, respectively.
In 1992, one study used isometric, isotonic, and isokinetic strength tests for evaluation after latissimus transfer. The authors concluded that forced extension is weaker only when the arms are in 60 degrees of flexion. There was no loss of range of motion. Another study done in 1995 reexamined change in muscle power and endurance after latissimus transfer. The authors concluded that women who underwent unilateral pedicled latissimus transfer showed a deficit of power and endurance in shoulder extension and adduction. This was seen in three specific work activities: ladder climbing, overhead painting, and pushing up from a chair. A more rapid onset of fatigue during prolonged activities involving these motions, including swimming, is noted.
A 45 year-old woman presents to your office several years following completion of her bilateral breast reconstruction. She is pleased with the appearance of her bilateral breasts statically, however she is dissatisfied with their dynamic appearance. Specifically, she states that she does not like how her implants are pushed laterally and flattened while at the gym doing exercises to strengthen her pectoralis major muscles. You astutely diagnosis the phenomenon she describes as “animation deformity.” Which of the following options provides the most definitive solution?
A) Injection of the bilateral pectoralis major muscles with botulinum toxin
B) Removal of the bilateral implants and replacement with autologous tissue
C) Removal of the bilateral implants and replacement with implants filled with a more cohesive gel
D) Thickening the mastectomy skin flaps with fat grafting
E) Changing the plane the implants are in from the subpectoral to the prepectoral plane
Correct answer is option E.
The patient is describing animation deformity, which refers to the tethering of the patient’s mastectomy flap skin to the underlying pectoralis major muscles, resulting in both visible contraction and lateral displacement of the entire breast mound/implant with any activation of the pectoralis muscle. Several strategies have been described for the treatment of animation deformity including injection of botulinum toxin to temporarily weaken the pectoralis major muscle, application of acellular dermal matrix (ADM) between the muscle and skin, and fat grafting between the muscle and skin. Although injection of botulinum toxin, its effect is temporary. The use of ADM or fat graft has had variable success and is not predictable. The best option is to remove the patient’s implants, reinsert the bilateral pectoralis major muscles to the chest wall, and replacement of the implants in the prepectoral plane.
A 43-year-old woman who is BRCA-positive is scheduled to undergo bilateral mastectomy. Tissue expander–based reconstruction is planned. Which of the following is the optimal duration of antibiotic prophylaxis for this patient?
A) No preoperative antibiotic
B) One preoperative antibiotic dose and another dose during skin closure
C) One preoperative antibiotic dose, followed by 24 hours of treatment while in the hospital
D) One preoperative antibiotic dose, followed by 24 hours of treatment while in the hospital and then discharge on oral antibiotics until drains are removed
E) One preoperative antibiotic dose, followed by 24 hours of treatment while in the hospital and then maintenance on oral antibiotics until tissue expanders are exchanged
The correct response is Option C.
The overall complication rate in breast reconstructive surgery is as high as 60%. Infection rates can exceed 20%, much higher than in clean elective surgery. The CDC guidelines suggest only 24 hours of peri-operative antibiotics beginning thirty minutes prior to skin incision. However, not all plastic surgeons agree with this. A 2013 meta-analysis found when comparing combined patient cohorts receiving no antibiotics, antibiotics for less than 24 hours, and antibiotics for greater than 24 hours, the average infection rates were 14.4, 5.8, and 5.8%, respectively. This demonstrated that the administration of antibiotics made a difference, however duration beyond 24 hours did not.
A study was published in 2013 evaluating the difference in surgical site infection between two different prophylactic antibiotic durations (24 hours and until drain removal). In this prospective, randomized, controlled non-inferiority trial, 24 hours of antibiotics is equivalent to extended oral antibiotics for surgical-site infection in tissue expander immediate breast reconstruction patients.
A 60-year-old woman with breast cancer is scheduled to undergo modified radical mastectomy followed by postoperative radiation therapy. Which of the following techniques will yield the most natural appearance of the breast with the fewest complications?
(A) Delayed reconstruction with an autologous tissue flap
(B) Delayed reconstruction with a tissue expander followed by implantation of a prosthesis
(C) Immediate reconstruction with an autologous tissue flap
(D) Immediate reconstruction with a tissue expander followed by implantation of a prosthesis
The correct response is Option A.
Reconstruction of the breast with a delayed (nonradiated) autologous tissue flap will yield the best breast appearance if postmastectomy chest radiation therapy is needed.
Radiation therapy negatively affects reconstructive outcomes with implants, causing a marked increase in capsular contracture and other complications. These complications are unrelated to the type of implant.
Totally autologous reconstruction is the best option for reconstruction of a radiated breast. In implant reconstruction of a radiated breast, the latissimus flap can be used to salvage tissue with periprosthetic contractures, particularly in a patient who is not a good candidate for a TRAM flap. The final outcome is not as good as that obtained with autologous tissue alone but can be acceptable.
In one study, patients who had immediate reconstruction with a TRAM flap followed by radiation therapy were compared with patients who had radiation therapy followed by delayed reconstruction with a TRAM flap. The study found that the incidence of late complications was significantly higher in the immediate reconstruction group than in the delayed reconstruction group. In fact, 28% of patients in the immediate reconstruction group required an additional flap to correct a distorted contour caused by flap shrinkage or severe flap contraction. These findings indicate that delayed reconstruction is preferred in patients who are candidates for breast reconstruction with a free TRAM flap and need postmastectomy radiation therapy.
A 45-year-old woman with a history of breast cancer presents for a discussion of breast reconstruction with silicone breast implants. She inquires about the current screening recommendations for implant rupture. Which of the following postoperative screening recommendations should the surgeon communicate to this patient?
A) CT scan at 3 years followed by CT, MRI, or ultrasound every 2 years thereafter
B) Mammogram every 5 years
C) MRI at 2 years then every 3 years thereafter
D) MRI at 3 years then every 2 years thereafter
E) MRI or ultrasound at 5 to 6 years then every 2 to 3 years thereafter
The correct response is Option E.
As a critically important part of the informed consent process, practitioners should be very familiar with updated information from the FDA. The screening recommendations for implant rupture for women with silicone gel-filled implants were recently updated (September 2020). The current FDA recommendations are that asymptomatic patients should have the implants evaluated with either ultrasound or MRI 5 to 6 years after implantation and then every 2 to 3 years thereafter. This new recommendation replaces the old recommendation by adding ultrasound as an accepted modality and extending the time until the first evaluation. The older recommendation was MRI evaluation at 3 years, with follow-up evaluation being performed every 2 years. These recommendations apply to women who have cosmetic augmentation and breast reconstruction. CT scan is not an acceptable modality for implant evaluation. Since this patient has had mastectomies and breast reconstruction, mammography is not indicated.
A 41-year-old woman comes to the office because of an invasive ductal carcinoma of the left breast. On mammography, the tumor is 3 cm from the nipple and measures 4 cm. A left-sided lateral periareolar scar extending from the 12 o’clock to the 3 o’clock position from a previous biopsy is noted. The patient wishes to undergo a nipple-sparing mastectomy. Which of the following findings places the patient at greatest oncologic risk, including risk for de novo or recurrent cancer or inadequate surgical margins, with this procedure?
A) Distance of tumor to nipple
B) Patient age
C) Presence of the periareolar scar
D) Size of tumor
E) Type of tumor
The correct response is Option D.
As surgical approaches to breast cancer treatment have evolved, nipple-sparing mastectomy (NSM) has emerged as an alternative to other approaches. It was initially used for prophylactic mastectomies, and patients reported increased satisfaction and body image with nipple-areola complex (NAC) preservation. The role of NSM has been expanded to therapeutic mastectomy, and with that there has been increased research in the oncologic safety of this approach.
Studies have evaluated therapeutic NSM in the context of invasive ductal carcinoma, invasive lobular carcinoma, and ductal carcinoma in situ. The type of cancer does not appear to be associated with the oncologic safety of NSM. Several studies have demonstrated an inverse association between NAC involvement and distance of the tumor from the nipple. While these studies have varied in their distance cutoffs, nipple involvement is reported to be over 50% when the tumor-nipple distance is less than 2 cm, as noted in one study. There is a direct correlation between tumor size and NAC involvement—the same study cited data that when the tumor was greater than 4 cm, the likelihood of nipple involvement was greater than 50%.
One published screening algorithm for plastic surgery includes tumor size less than 3 cm, and tumor location greater than 2 cm from the nipple as criteria for NSM candidacy.
A periareolar scar, if large, may compromise the blood supply to the NAC. Acceptable incisions for NSM, however, include a periareolar incision of 25 to 50%.
A 43-year-old woman would like to discuss plans for breast reconstruction after her upcoming unilateral mastectomy. Postoperative radiation therapy is planned. Which of the following is the most likely benefit of tissue expander–based breast reconstruction compared with immediate autologous breast reconstruction using this patient’s abdominal tissue?
A) Better symmetry
B) Improved postoperative sensation
C) A larger, more ptotic breast reconstruction
D) Lower risk of complications from radiation
E) Preservation of the patient’s options for final reconstruction.
Correct answer is option E.
Immediate breast reconstruction with tissue expanders followed by reconstruction of choice preserves the patient’s skin envelope and keeps open options for definitive final reconstruction of choice whether with an implant or autologous tissue.Tissue expander-based reconstruction is associated with a higher complication rate inthe setting of radiation therapy but preserves abdominal and back tissue as options forautologous reconstruction. Implant-based reconstruction does not provide theadvantages of improved symmetry, sensation, or breast ptosis
A 55-year-old woman with no significant past medical history is scheduled for an immediate free transverse rectus abdominis myocutaneous (TRAM) flap reconstruction following a mastectomy for breast cancer. The plastic surgery resident suggests starting a therapeutic dose of intravenous heparin postoperatively to improve flap survival.
Based on current evidence, what is the most likely outcome of routinely using therapeutic anticoagulation in this patient?
a) A significant reduction in the rate of microvascular thrombosis and improved flap survival
b) A significant increase in hematoma formation with no proven benefit in flap survival
c) A decreased incidence of fat necrosis within the flap
d) Protection against systemic thromboembolic events with no change in flap outcomes
e) A reduction in both hematoma rate and flap failure
The correct answer is option B.
Multiple systematic reviews and meta-analyses have consistently shown that the routine use of therapeutic anticoagulation (like heparin) in free flap surgery does not confer a protective benefit. It does not reduce the rate of microvascular thrombosis or improve flap survival (making options A and E incorrect). Instead, it significantly increases the risk of postoperative hematoma and bleeding complications. Therapeutic anticoagulation is not indicated for routine cases but may be considered on a case-by-case basis for flap salvage or in patients with a known hypercoagulable disorder. The incidence of fat necrosis (option C) is not decreased by systemic anticoagulation.
References:
Lee KT, Mun GH. The efficacy of postoperative antithrombotics in free flap surgery: a systematic review and meta-analysis. Plast Reconstr Surg. 2015;135(4):1124-1139. doi:10.1097/PRS.0000000000001100
Jakobsson S, Kamali A, Edsander Nord Å, Sommar P, Halle M. Free flap surgery outcome related to antithrombotic treatment regime: an analysis of 1000 cases. Plast Reconstr Surg Glob Open. 2021;9(12):e3961. doi:10.1097/GOX.0000000000003961
Dawoud BES, Kent S, Tabbenor O, Markose G, Java K, Kyzas P. Does anticoagulation improve outcomes of microvascular free flap reconstruction following head and neck surgery: a systematic review and meta-analysis. Br J Oral Maxillofac Surg. 2022;60(10):1292-1302. doi:10.1016/j.bjoms.2022.07.016
A 41-year-old man is referred to the office because of a mass on his left breast that has been growing rapidly for 1 month. Examination of the specimen obtained on core needle biopsy confirms invasive mammary carcinoma. Genetic testing results are positive for BRCA2. In addition to an increased risk of male breast cancer, which of the following other types of cancer is most likely to be associated with this patient?
A) Colon
B) Lung
C) Pancreatic
D) Renal
E) Thyroid
The correct response is Option C.
Men with harmful BRCA1 mutations also have an increased risk of breast cancer and, possibly, pancreatic cancer, testicular cancer, and early onset prostate cancer. However, male breast cancer, pancreatic cancer, and prostate cancer appear to be more strongly associated with BRCA2 gene mutations. Colon, lung, renal, and thyroid cancers are not associated with the BRCA1 and BRCA2 gene mutations.

A 43-year-old woman is scheduled for reconstruction of the right breast with a latissimus dorsi flap. She is at greatest risk for which of the following complications?
(A) Chronic chest wall pain
(B) Dorsal wound dehiscence
(C) Partial flap necrosis
(D) Seroma
(E) Stiffness in the ipsilateral shoulder
The correct response is Option D.
The most common complication in the scenario described is seroma formation, which is estimated to be as high as 35% to 60%. Other less common complications include chest wall pain (6%), dorsal wound dehiscence (4%), partial flap necrosis (1-7%), and shoulder stiffness (1%).
A 40-year-old woman is scheduled to undergo reconstruction of the right breast via a free TRAM flap. She has smoked two packs of cigarettes daily for the past eight years. This patient’s smoking history increases her risk of which of the following postoperative complications?
(A) Hematoma
(B) Mastectomy flap necrosis
(C) Seroma
(D) TRAM flap loss
(E) Vessel thrombosis
The correct response is Option B.
One study found no significant increased risk of flap loss, vessel thrombosis, or fat necrosis in free TRAM flaps performed on smokers. However, smokers did have an increased risk over their nonsmoking counterparts in the area of mastectomy skin flap necrosis, abdominal hernia, and abdominal flap necrosis.
Another study of 569 free TRAM flaps found that smokers had an increased rate of fat necrosis, wound infection, abdominal flap necrosis, and mastectomy flap necrosis. There was no correlation with free flap loss, thrombosis, hematoma, or seroma.
By using the deep inferior epigastric vessels, which are the primary blood supply to the TRAM flap, risks to the flap itself are minimized even in smokers. But smoking continues to increase the risk of donor site morbidity and native breast skin necrosis.
An otherwise healthy 41-year-old woman is scheduled to have bilateral prophylactic NSM for a BRCA1 mutation. Which of the following is an advantage of prepectoral implant reconstruction when compared with submuscular implant reconstruction?
A) There are significantly more acute postoperative surgical complications
B) There is a higher revision rate
C) There is a lower rate of animation deformity
D) There is a lower rate of upper pole rippling and implant palpability
E) There is more pain and functional impairment
The correct response is Option C.
The patient is a young, healthy, thin woman presenting for bilateral breast reconstruction following prophylactic mastectomies because of increased lifetime risk of breast cancer. She will maintain her entire breast skin envelope because she has planned nipple-sparing mastectomies and does not wish to increase her breast size with the operation. She has questions about the plane of implant placement above or below the pectoralis muscle and the answer choices provide the opportunity to counsel her on direct to implant versus staged expander to implant breast reconstruction.
Because of the lack of camouflage afforded by placement of the pectoralis muscle over the upper pole of the breast implant, prepectoral breast reconstruction is associated with increased rippling of the upper portion of the breast. This patient is thin according to BMI and so will have an increased risk of upper pole rippling that can be improved with subsequent fat grafting, provided she has adequate donor sites for fat harvest.
Several patient series reporting on early outcomes after prepectoral breast reconstruction have used a partially submuscular patient cohort as a comparison for acute postoperative complications. The overwhelming majority of these series showed no significant differences in acute postoperative outcomes and revision rates between techniques.
Postoperative functional assessments have demonstrated less pain and earlier return of function after prepectoral implant placement compared to submuscular implant placement. Re-siting of submuscular implants to a prepectoral plane have demonstrated resolution of animation deformity.
Algorithms for patient selection have slowly evolved over the past five years with the only constant recommendation being that the ideal candidate has a BMI less than 30 kg/m2. Earlier series emphasized mastectomy skin flap thickness, whereas more recent studies focus on skin flap viability. Earlier studies considered radiation treatment a contraindication, whereas more recent reports demonstrate the negative impact of radiation on pectoralis major fibrosis in submuscular reconstruction as compared with prepectoral implant placement.
An otherwise healthy 54-year-old perimenopausal woman is scheduled for a mastectomy for biopsy-proven right-sided grade 2 ductal carcinoma. According to the National Comprehensive Cancer Network (NCCN) guidelines, postmastectomy radiation therapy will be the standard of care for this patient if she has which of the following surgical outcomes?
A) 1-cm surgical margins, four positive axillary lymph nodes
B) 1-cm surgical margins, one positive axillary sentinel node
C) 1-mm surgical margins, no positive axillary nodes
D) 5-mm surgical margins, no positive axillary nodes
E) 5-mm surgical margins, three positive axillary nodes
The correct response is Option A.
Traditionally, the need for radiation therapy has been a contraindication for implant-based reconstruction, and autologous reconstruction is the conservative gold standard for women with advanced cancer needing postmastectomy radiation. More recently, there have been reports of successful implant based reconstruction in the setting of postmastectomy radiation that have similar complication profiles and good oncologic outcomes compared with autologous reconstruction. Protocols vary between those that radiate the expander and then expand, and those that expand and then radiate the permanent implant. Being able to anticipate which patient will require postmastectomy radiation is essential for joint decision making about breast reconstruction with the patient prior to her mastectomy.
By National Comprehensive Cancer Network (NCCN) guidelines, relative indications for postmastectomy radiation therapy include: positive sentinel node with unknown status of other axillary nodes, one to three positive nodes on permanent histology, and close surgical margins (less than 5 mm). Postmastectomy radiation is recommended as the standard of care in the situations of positive surgical margins with the inability to get clear margins and four or more positive lymph nodes.
A 52-year-old woman receives a diagnosis of invasive ductal carcinoma of the right breast. Which of the following details from this patient’s history is the strongest risk factor for this diagnosis?
A) Early first pregnancy (less than 30 years)
B) Early menarche (less than 12 years)
C) Early menopause (less than 55 years)
D) Multiple episodes of breast-feeding
E) Remote oral contraceptive use
The correct response is Option B.
Early menarche is the highest risk factor for breast cancer of the options listed. Late first pregnancy, late menopause, no breast-feeding, and recent oral contraceptive use are also risk factors for breast cancer but are not as high risk.
A 55-year-old female has received a right unilateral mastectomy and immediate reconstruction with a free DIEP flap. The DIEP flap was designed so that the only visible abdominal skin of the flap is located as a central circular paddle, where the areola and nipple originally were. Her native left breast is symmetric in size and position compared to the reconstructed right breast mound. Her left nipple has 2 cm of projection. She now wishes to undergo nipple reconstruction; however, she does not want to change the dimensions of her right reconstructed breast, specifically she wants to maintain as much projection as possible. What is the best option for her nipple reconstruction?
A) C-V flap
B) Double-opposing tab flap
C) Thomas Flap
D) Nipple-sharing graft
Correct answer is option D.
The CV, double opposing tab, and Thomas flaps all result in a variable loss of projection when the local flap’s donor site is closed. This must be discussed with the patient preoperatively. This particular patient has a very projecting nipple on the left native breast. In this situation, The distal 1 cm of the left nipple can be amputated and transferred to the right breast mound as a full thickness graft. The left nipple donor site can be closed with a few interrupted absorbable sutures. Of the techniques listed, the nipple sharing method would be most optimal given this patient’s concerns about changing the dimensions of her right breast mound.
For reconstruction mammaplasty, which of the following is an advantage of the extended latissimus dorsi flap over the standard latissimus dorsi myocutaneous flap?
(A) Better flap perfusion
(B) Decreased need for breast implant
(C) Fewer donor-site seroma
(D) Less sacrifice of latissimus dorsi muscle
(E) Smaller donor-site scar
The correct response is Option B.
The latissimus dorsi (LD) myocutaneous flap was one of the first methods of breast reconstruction ever described. However, with the increasing popularity of transverse rectus abdominis myocutaneous (TRAM) flap breast reconstruction, for many, the LD flap has become a secondary choice for autologous breast reconstruction. One reason for this has been that the standard LD flap alone often does not provide sufficient volume for breast reconstruction. In fact, it is a common practice to combine the LD flap with a prosthesis to achieve adequate breast volume.
Variations of the LD flap have been described to increase its volume and avoid the addition of a prosthesis. The first “extended” LD (ELD) flap was described by Hokin in 1983 and included lumbar fat extensions of the LD flap. Others have used the buried de-epithelialized LD myocutaneous flap for breast reconstruction. McCraw and Papp modified this technique by using a fleur-de-lis skin paddle design to carry additional fat on the surface of the LD muscle, creating the totally autogenous LD breast reconstruction.
The design of the ELD flap has evolved to include the parascapular and scapular “fat fascia” in addition to the lumbar fat for additional volume. The main advantage of the ELD flap is that it can provide autogenous tissue to replace breast volume without an implant and with acceptable donor site contour and scar. Because the ELD flap transports additional tissue from the back so a breast prosthesis is not required, this avoids all potential problems associated with implants, e.g., development of capsular contracture and deformation of the reconstructed breast.
With ELD flaps, donor site complications, including seroma formation and wound necrosis, can be a significant problem.
What is the optimal timing for an office-based nipple-areolar reconstruction?
A) Immediately, at the time of mastectomy and immediate reconstruction
B) During the second stage of a two-stage expander-implant reconstruction
C) At the time of the first postoperative appointment, 2 weeks following the second stage of a two-stage expander-implant reconstruction
D) 3-4 months following the completion of all breast mount operative revisions
Correct answer is option D.
The timing of nipple-areola reconstruction must be carefully considered. Nipple-areolar reconstruction may be performed safely with small revisions (limited fat grafting, scar revision, etc) that do not alter the stable configuration of the underlying breast reconstruction. Ideally, the breast mound should be an aesthetic and symmetric position on the chest wall and the patient must be happy with the volume of the breast mound prior to nipple areolar reconstruction. Every effort should be made for nipple-areolar reconstruction to be the last step in the reconstruction.
A 39-year-old woman with a history of fibrocystic breast lesions comes to the office for consultation. She has no family history of breast cancer. Results of routine mammograms have been negative; she has never undergone biopsy. Which of the following is the most appropriate recommendation for this patient regarding managing her risk of breast cancer?
A) Continue to schedule routine mammograms
B) Refer for mastectomy
C) Schedule core needle biopsy
D) Schedule fine-needle aspiration
E) Schedule genetic testing
The correct response is Option A.
Studies have shown the fibrocystic changes alone in the breast are not directly linked to an increased risk of breast cancer, so there is no indication for fine-needle aspiration or core biopsy. Cancer risk increases in benign breast disease with increased proliferation and atypical hyperplasia. Even with no family history of breast cancer, it is recommended that the patient continue routine mammograms. Fibrocystic breast disease has not been linked in the literature to an increased risk of mutations of the BRCA genes; therefore, genetic testing is unnecessary.
A 33-year-old woman comes to the office with a 6-cm rapidly growing tumor of the left breast. She wears a size 36C brassiere. The tumor has a bluish hue and skin veins are dilated. A phyllodes tumor is diagnosed, and surgical excision is planned. Which of the following is the most appropriate surgical procedure to treat this patient?
A) Excision with 1-cm margin
B) Excision with 2-cm margin
C) Excisional biopsy
D) Modified radical mastectomy
E) Radical mastectomy
The correct response is Option A.
Phyllodes are large benign tumors that occur primarily in the perimenopausal patient. Previously, they were referred to as cystosarcoma phyllodes, a term coined in 1838 because the tumors are fleshy and have a gross leaf-like intracanalicular growth pattern. However, this is a misnomer because these tumors do not behave like sarcomas and are rarely malignant. The histologic characteristics that separate fibroadenomas from phyllodes tumors are not well defined and have been somewhat controversial. Nevertheless, phyllodes tumors typically are large fibroadenomas that histologically have more stromal cellularity than that seen in the typical fibroadenoma. The classification of benign versus malignant phyllodes tumors is not sharply delineated, and the term borderline lesion may be more appropriate. Borderline lesions have more mitoses per high-power field and moderate nuclear pleomorphism. They have a tendency to recur after local excision but do not demonstrate true malignant behavior. When metastases of a phyllodes tumor have been reported, there have been obvious sarcomatous elements such as liposarcoma or rhabdomyosarcoma in the lesion.
The surgical treatment of phyllodes tumors has recently been redefined. In the past, simple or radical mastectomies were recommended for the treatment of large phyllodes tumors. Currently, most surgeons perform more conservative surgery. Several clinical studies have recommended the excision of tumors with 1-cm clear margins or mastectomy if breast conservation is impossible.
An otherwise healthy 37-year-old woman presents for delayed microsurgical breast reconstruction. Which of the following is associated with use of tamoxifen?
A) Hemodynamic instability
B) Impaired wound healing
C) Increased bleeding
D) Seroma formation
E) Thromboembolic events
The correct response is Option E.
Breast cancers that are estrogen receptor positive may be responsive to adjuvant chemotherapy with selective estrogen receptor modulators such as tamoxifen, which can reduce recurrence and mortality. Tamoxifen is associated with thromboembolic events, such as deep venous thrombosis and pulmonary embolism. This prothrombotic effect has been postulated to be secondary to the effect of tamoxifen on estrogen receptors that are abundant within vascular endothelium.
Tamoxifen has been shown to be associated with increased rates of total flap loss and decreased rates of flap salvage when taken within 28 days of microsurgical breast reconstruction, which represents two half-lives of the active metabolite of tamoxifen (N-desmethyl tamoxifen, t1/2=14 days). It has therefore been recommended that in patients undergoing microsurgical breast reconstruction, tamoxifen be held for at least 28 days preoperatively. Some authors have further advised holding the medication postoperatively in addition to preoperatively.
Tamoxifen is not associated with impaired wound healing, increased bleeding, hemodynamic instability, or seroma formation.
A 45-year-old woman is scheduled to undergo mastectomy of the right breast followed by reconstruction using a free TRAM flap. She has a 15 pack/year history of cigarette smoking. This patient is at increased risk for development of each of the following postoperative complications EXCEPT
(A) abdominal flap necrosis
(B) fat necrosis
(C) hernia
(D) mastectomy skin flap necrosis
The correct response is Option B.
The free TRAM flap is frequently advocated for breast reconstruction in high-risk patients, including those who smoke, because of its enhanced blood supply; however, patients who smoke are still at increased risk for development of complications. One large retrospective study showed that patients who smoked were at greater risk for developing hernia and necrosis of the mastectomy skin flap and abdominal flap when compared with nonsmokers undergoing breast reconstruction with the free TRAM flap. Because patients who had a 10 pack/year or greater history of smoking were at greatest risk for perioperative complications, it has been suggested that reconstruction should be delayed until the patient has stopped smoking for at least four weeks. Studies have shown no significant increase in the rate of fat necrosis, flap loss, or vessel thrombosis in patients who smoked when compared with nonsmokers.
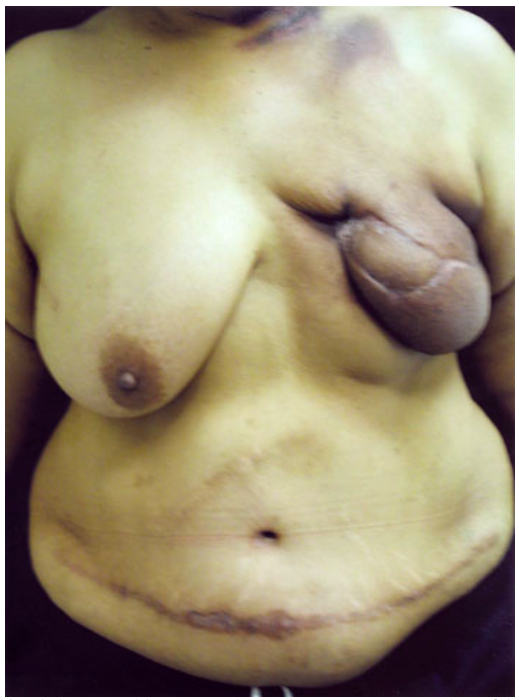
A 45-year-old woman who underwent reconstruction of the left breast with a TRAM flap followed by radiation two years ago is evaluated for a second reconstruction procedure on the left breast (shown). She requests that only reconstruction with her own tissues be performed and is opposed to surgery of the right breast to restore symmetry. On physical examination, the breast is shrunken and firm. After removal of the unsalvageable left breast, which of the following is the most appropriate reconstruction technique at this time?
(A) Deep inferior epigastric perforator (DIEP) flap
(B) Free TRAM flap
(C) Latissimus dorsi myocutaneous flap
(D) Superior gluteal artery perforator (SGAP) flap
(E) Thoracoepigastric flap
The correct response is Option D.
When there is near-total loss of a TRAM flap for breast reconstruction, it is important that a second breast reconstruction procedure be successful, with special consideration for safety. When there is insufficient lower abdominal tissue for tissue expansion and transfer of a second flap, neither a free TRAM flap nor a deep inferior epigastric perforator (DIEP) flap recruiting soft tissue in the same lower abdominal areas is an option. A latissimus dorsi myocutaneous flap is a reliable source of autogenous tissue; however, considering the size of the contralateral breast in this patient, a latissimus dorsi myocutaneous flap would need to be supplemented by a permanent expander implant to provide sufficient volume. A staged breast reconstruction with tissue expander would also require permanent implantation of a prosthesis upon completion of the expansion process. A gluteus free flap is considered when the latissimus dorsi flap is not sufficient or available and the patient requests autogenous tissue breast reconstruction. The free sensate superior gluteal artery perforator (SGAP) flap is a free sensate flap based on the superior gluteal artery perforator. It has an abundance of adipose tissue (specimens up to 760 g), even in thin patients, a relatively long vascular pedicle, a discrete scar, improved projection compared with the DIEP and TRAM flaps, and preservation of the entire gluteus maximus muscle with extremely low donor site morbidity.

















-
Anesthetics - Critical Care152
-
Basic Surgical Principles203
-
Blepharoplasty - Oculoplastic105
-
Body Contour - Abdominoplasty - Liposuction184
-
Breast Augmentation, Mastopexy182
-
Breast Reconstruction177
-
Breast Reduction / Gynecomastia81
-
Burns principles and treatment136
-
Chest/Abdomen/Trunk/Rec/Congenital193
-
CL & CP, CL Nose, VPI161
-
Coding27
-
Craniofacial Anomalies - Migraine212
-
Ear Reconstruction - Microtia - Trauma118
-
Oculoplastic - Eyelid Reconstruction38
-
Facelift - Browlift110
-
Facial Palsy - Cheek and Lip reconstruction77
-
Facial Rejuvenation - Chemical Peel / Fillers / Botox / Non-Surgical115
-
Facial Trauma - OMF - Mandible171
-
Flaps - Principles - Complex Flap Recons.151
-
Genital, Urinary, Gender Affirmation, Pelvic52
-
Grafts: Skin, Fat, Cartilage and Bone97
-
Hand & Lower Extremities - General75
-
Hand - Amputation, Replantation, Dupuytren's235
-
Hand - Arthritis47
-
Hand - Extensor and Flexor Tendon Injury147
-
Hand - Fractures - Dislocations77
-
Hand - Limbs - Congenital105
-
Hand Nerve Injury - Compression - Brachial plexus198
-
Hand - Tumors77
-
Hand - Wrist ligament injuries and fractures97
-
Head and Neck Anatomy - Embryology76
-
Head and Neck Congenital105
-
Head and Neck Tumors / Parotid156
-
Infections - Soft Tissue - Hand106
-
Lasers50
-
Lower Extremity218
-
Lymphedema / venous Inssuficiency43
-
Mandible - OMF93
-
Microsurgery principles51
-
Nasal Reconstruction52
-
Orthognathic, TMJ, Chin138
-
Practice management - Health Care System - Ethics - Legal - Research79
-
Pressure Injuries55
-
Rhinoplasty - Septoplasty127
-
Scalp, Forehead, Cranial Reconstruction - Hair Restoration48
-
Skin Lesions Benign, Malignant SCC BCC (No-melanoma)158
-
Skin Melanoma45
-
Tissue Expansion18
-
Wound Healing, Hypertrophic scars and Keloids, Transplant125
-
Vascular Tumors And Malformations - PAD - Trauma111
