Define autonomy.
Autonomy involves: - Acting with sufficient understanding. - Acting freely from the will of others. - Acting in accordance with your own (enduring) values.
Why is autonomy important?
Consequentialist view – respecting autonomy generally leads to better outcomes because the patient is more involved with their own healthcare, and are more likely to trust the doctor, feel satisfied and stick to the prescribed regimen (if there is one).
Deontological view – it is a requirement according to the GMC, and therefore is right and important in itself. Kant argues that we should respect autonomy because we treat people as ends, not means.
Virtue ethics – a virtuous person would allow an individual to be self-determinant.
In clinical practice, what is the significance of autonomy?
- Enabling patients to come to informed decisions about their treatment voluntarily. - Respecting patient’s wishes regarding requests for and refusals for treatment. Indeed, the patient’s right to refuse treatment is protected by the law. Doctors can refuse to give a treatment, however. - Even if not acting in accordance with patient wishes, due consideration should be taken and the patient should be informed as to why.
What should be taken into consideration when assessing a patients best interests?
When doctors act in a patients best interests they are acting in ways that will have an overall net benefit for the patient. This obviously links in with beneficence (acting in ways the benefit the patient). Non-maleficence states that it is important not to do any harm to the patient, however often a treatment will have unwanted side effects but is deemed to be in the best interests of the patient because of the overall net positive effect.
How would you evaluate the best interests of a patient?
Clearly medical expertise is often needed when evaluating a patient’s best interests (e.g. whether a treatment is clinically indicated). But it is important to recognise that no best interests assessment can be made without a proper understanding of the needs, priorities, concerns and values of individual patients, and this will very often require going far beyond what medical expertise alone can tell us. Indeed, when evaluating the interests of a patient medical practitioners will often have to inquire into the psychosocial factors relevant to a patient, including occupation and lifestyle, as well as such things as patients’ priorities, concerns and expectations (hence, the need to consult patients regarding factors relevant to their interests).
What are the difficulties faced when assessing the patients best interests?
- When the patient cannot communicate. - When trying to weigh up conflicting goods. - Your own values might distort what you think is in the patients best interests. - The patient might disagree with what you think is in their best interests. - The future can be difficult to predict. Could an intervention deemed to be in the patients best interests now, become negative in the future? - Best interests is a value-laden term and somewhat subjective. Respecting patient autonomy and acting in their best interests are important, and respecting autonomy is the best outcome because patients themselves often known inherently what is good for them. This is not always the case though.
What are the criteria for patient-centred care?
- Explores the main reason for the visit, concerns and needs for information. - Seeks an integrated understanding of the patients world - their whole person, their needs and life issues. - Finds common ground on what the problem is and mutual agreement on management. - Enhances prevention and health promotion. - Enhances the continuing relationship between the patient and doctor. - Is realistic.
What model does Patient Centred Care replace?
The conventional medical model (or biomedical model) - an old fashioned, paternalistic view of medical practice where it is assumed that the patient knows little and the doctor knows best, so go along with what the doctor says.
What assumptions are made in the biomedical model?
- It assumes disease to be fully accounted for by deviations from the norm of measurable biological (somatic) variables. - Leaves no room for psychological and behavioural dimensions. - Essentially assumes that we are all the same and will experience illness in the same way.
How would you explore the disease (biomedical) and illness (psychosocial) experience of a condition?
Disease - History, Physical Exam, Investigations. Illness - Ideas, Concerns, Functions and Expectations. (SOCRATES). The context in which they live family, finances, education, leisure, social support, culture, media Finding common ground – problems and priorities, goals of treatment / management, roles of patient and roles of doctor Incorporating prevention and promotion – health enhancement, risk avoidance and reduction, early identification, complication reduction Being realistic involves time and timing, team building and teamwork and an awareness of resource constraints Patients want doctors who are biomedically competent, but they also want to be treated individually and respect. Hippocrates states that the role of medicine is ‘to cure sometimes, to relieve often and to comfort always.
What factors influence the way people perceive their symptoms?
Gender - men are statistically less likely to consult a doctor. Race/Ethnicity - Different ethnic groups may consider illnesses and symptoms in different ways, affecting their decisions to consult medical professionals. For example, many west africans don’t believe that ebola is real and aren’t consulting health care professionals. Class - working class individuals tend to seek help less than other classes, adopting practical definitions of health (i.e. only recognising illnesses if they affect the individuals ability to do something). Age - younger people see illness as not being fit, whereas older people see it as not being functional and are more likely to seek help.
What are the barriers to help-seeking behaviour?
- Availability and provision of healthcare - Attitude of health care professionals - Social distance. - Geographical distance - Cost of care (cost vs benefit). - Availability of transport - Bad experiences - Waiting times - Loss of earnings, childcare, time and effort. - Inverse care law (areas that have the most need for healthcare have the least available and vice versa).
Explain how the internet influences help-seeking behaviour.
- Patients can check symptoms to see if they need medical attention. - Build up the confidence to ask questions. - Clarifications of doctor’s advice (esp re: medication). - Social support (especially re: chronic illness) - Self management and feelings of being in control of disease.
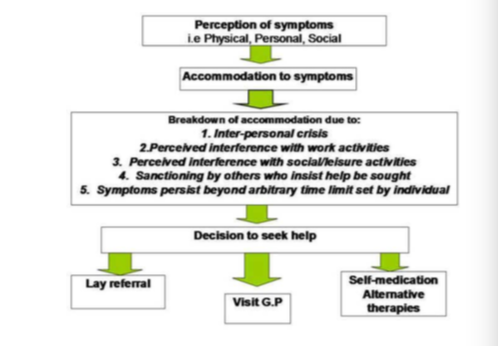
Explain Zola’s help-seeking model.
Zola’s model states that people first try to accommodate symptoms, and only seek help due to one or more of five triggers including:
Give some facts about the Lay Referral System
- Prior to going to a GP 70% of patients consulted more than 3 lay people
- Social context can play a large role in whether people consult others (e.g. closed communities, or women who talk to relatives a lot are more likely to consult).
- Commonly relatives, pharmacists, NHS direct and the internet are consulted.
Explain how self-medication is becoming more important.
Individuals are becoming increasingly more knowledgable about their own health as a result of the information being much widely available with the advent of the internet etc.
More and more people are buying GSL drugs (as opposed to POM) from the supermarket or pharmacy to relieve their symptoms.
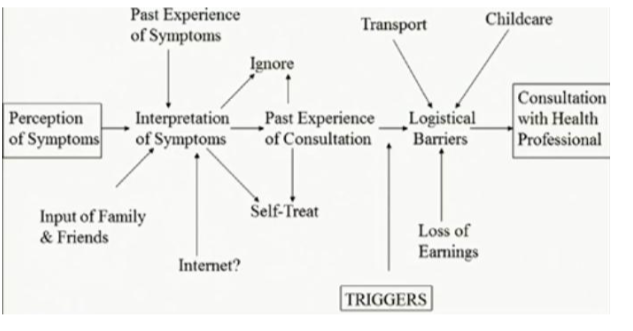
Give an diagramatic overview of help-seeking behaviour and illness perception.
Explain the term ‘Symptom Iceberg’
The notion of the symptom iceberg is that symptoms per se do not prompt a visit to the doctor. Most health care work is done by lay people.
What is Illness Behaviour?
Explains the process of seeking help.
The ways in which symptoms may be differentially perceieved, evaluated and acted upon (or not acted upon) by different kinds of persons. Illness behaviour is a culturally learned response (not an automatic response for a given illness).
Isn’t just individual, but socially pattered and might vary by gender, age, social class (symptoms may be part of everyday life; working class have functional definitions of health; middle class experiential and expansive definitions), race (irish are stoical, italian or jewish are more expressive), culture.
What are some common help seeking tiggers?
- Interference with work or physical activity.
- Interference with social relations.
- Interpersonal crisis.
- Time limit on symptoms
- Sanctioning.
What are the common pathways of patient care in the information age?
- Can check if symptoms warrant medical attention.
- Increased confidence to ask questions.
- Clarification of doctors advice (e.g. about medication).
- Social support.
- Self-management and feeling of being in control over illness.
- Still relying and trusting doctors.
- Shared decision making (PCC).
What are the common barriers to help-seeking?
- Provision and availability of services.
- Attitudes of healthcare staff.
- Social/cultural distance.
- Inverse care law.
- Geogrpahical distance.
- Time, effort, childcare, loss in earnings.
- Car ownership.
- Transport costs and availability.
- Cost vs Benefits
- Bad experiences
- Waiting times.
