What is ‘downstream’ and ‘upstream’?
Downstream - the disease and curative treatment. Upstream - looking at the causative agent and preventing disease from ever occurring. Doctors primarily focus on the downstream, but also promote health. There are vested interests in the downstream which prevent health promotion and prevention from developing (e.g. companies that make drugs, medical equipment, controversy of closing hospitals in politics etc.)
Describe the epidemiological transition in communicable diseases.
In the mid 19th century, communicable diseases accounted for 75% of all deaths. In the later 20th century, that figure fell to 2%.
Compare the epidemiology of diseases in wealthy nations vs poorer nations.
The characteristic of epidemiological transition in wealthy nations is a fall in infectious diseases and a rise in chronic, non-communicable diseases. Known as ‘diseases of affluence’ because they affect wealthy nations. However, they disproportionately affect the poor in those nations.
What factors are determinants of health outcomes?
- Social and economic (education, housing, employment, poverty, income). - Environment (air quality, pollution, water, transport, climate change). - Lifestyle issues (diet, smoking, drug misuse, excersise). - Health Services (delivery and access, developments in medicine, diagnosis, rehabilitation).
Briefly define health promotion.
The process of enabling people to increase control over, and improve, their health. It moves beyond focus on individual behaviour towards a wide range of social and environmental interventions.
What are the WHO’s 5 aspects of health promotion.
Healthy public policy - by this they mean the health consequences or ‘health impacts’ of ALL areas of policy (education, transport, housing) should be taken into account by policy makers • Supportive environments - action needs to be taken to improve the settings in which people live their everyday lives e.g in home design and safety issues (accidents); workplace – e.g smoke free work places, or working towards sustainable environments • Community action - this is when groups of people, e.g. in a community take action to improve health for example campaign against local pollution or traffic hazzards. • Personal skills - this is about helping individuals to develop life skills which better enable them to deal with health issues e.g stress management, self esteem and so on. • Reorienting health services - this is about shifting the balance of resource from treatment to prevention – trying to ensure a population approach to health care rather than one that is overly individualist.
Define ‘Health Education’
Health education is a type of health promotion. It is any combination of learning experiences that facilitate actions that are conductive to health. Aims to give people knowledge and skills to change potentially health damaging behaviour e.g. advice from health professionals, mass media campaigns.
Define ‘Health protection’
Health protections refers to more legislative approaches to protect public health at a population level, e.g. smoking ban, seat belts etc.
Define primary, secondary and tertiary forms of disease prevention.
Primary Prevention: prevent onset of disease by health promotion (health education and health protection) and screening for risk factors. - Secondary Prevention: detection and cure of a disease at an early stage. - Tertiary Prevention: Preventing a disease from getting worse and minimising effects by symptom management, palliative care etc.
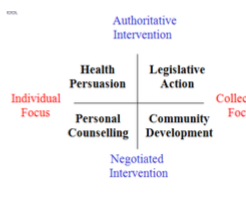
Summarise Beatties typology for different approaches to health promotion.
There are some dilemmas associated with health promotion and the shift from treatment to prevention. What are they?
- The opportunity cost. Resources are already scarce and people are dying of disease. Why should we divert resources upstream to promote health instead putting more effort into helping those afflicted with the disease?
- It is difficult to determine what is effective and what is ineffective because social changes aren’t easily testable in randomised control trials, as effects are often long term, hard to measure and confounding factors difficult to control. Should we assign any resources to health promotion if there is no proof it will work?
- Balance of individual liberty and protection of public health
- Who is responsible for health? Individual? Community? Health service? Government?
Ideally, when thinking about promoting health, we should find the best balance of autonomy, beneficience, non-maleficence and justice.
You’re a doctor and you’re about to engage in some health advice to a patient in order to engage in opportunistic prevention. What guidelines should you follow when talking to patients?
- Awareness of patient’s receptiveness.
- Respectful - listen to the patients views.
- Avoid preaching
- Caring not scaring
-
If individual freedom (autonomy) is important, should the right to treatment be? Should those who take risks (i.e. smoking) be denied treatment?
Argument For:
- Smoking led to disease
- Smoking will limit the effectiveness of surgical intervention.
- Poor outcome will result more surgery
- Expensive when resources are limited - must target where most effective.
Arguments Against:
- Doctors have ethical obligation to treat on basis of need and best available treatment.
- ‘Slippery slope’ - should we also deny treatment to those who self-harm?
- Poor people smoke more than rich people.
- Value judgements - deserving and undeserving.
What is the signiciance of the prevention paradox?
‘A preventative measure which brings much benefit to the population offers little benefit to each participating individual’
For example: increasing tax on alcohol and cigarette - collective effect is less alcohol is consumed, but the individual still buys alcohol.
What practical ways can doctors do to promote health?
- Individual consultationa advice.
- Institutional context (working with other agencies to promote health - HPA, WHO).
- Political and social clout.
What socioeconomic measures are indicative of general health?
- Highest educational attainment
- Occupational status (employed, manegarial, skilled, unskilled)
- Housing/tenure (owner or occupier?)
- Area deprivation - IMd.
Due to industrialisation, general health of the UK population improved across all social classes. Death rates due to infecitous diseases declined and more children survived into adulthood.
However, death rates amongst those in lower social classes are still higher. What explanations are there for this inequality in health, according to the Black Report of 1982.
- It is a statistical artefact (not real).
- Peoples health drives their social class (health related social mobility).
- Result of differences in health behaviour.
- Result of broader social inequalities in people’s lives.
The idea of inequalities in health being statistical artefacts doesn’t hold much water, as the statistical limitations in the data are not sufficient to account for such vast inequalities. The idea that people’s health drives their social class is important at an individual level but not very important at a societal, population level – only making a modest contribution to the gradient.
The idea that it is due to differences in health behaviour has strong evidence. Health- damaging lifestyles (smoking, drinking, bad diet) are socially patterned. But these behaviours are shaped by peoples circumstances and are therefore inseparable from the fourth explanation, which is that social inequalities cause health inequalities. This idea sees health as determined by social structure (position into which you were born). This influences their material conditions (physical environment you live in, where you work etc). These everyday material conditions influence health directly (hazardous exposures, stress, unemployment, low pay etc) as well as indirectly by shaping their lifestyle (diet, smoking, drinking etc).
Childhood circumstances are also a big predictor of health inequality. Why is this?
- Circumstances across life matter for your health - but circumstances in early life are particularly important.
- This is because childhood is a period of very rapid development and heightened sensitivity to environmental influences - i.e. biological and psychological impact of everyday circumstances is greater than at other periods of life.
- Poor circumstances can therefore have life-long effects.
Define prevalance and incidence.
Prevalence is the percentage of individuals who have a condition at a point in time out of the entire population at that time, given by
P = no. of individuals having disease at a specific time / number of individuals in the population at that point in time.
Incidence is the rate of development of a disease in population over a given amount of time.
In research, what is the hierachy of evidence?
- Sysematic reviews and meta-analyses
- Randomised control trials
- Cohort studies (controlled observational studies)
- Case control studies (controlled observational studies).
- Case series
- Case report (uncontrolled observational study)
- Ideas and opinions.
- Animal research.
- In vitro research.
What words would a patient use to describe GI symptoms?
- Difficulty swallowing.
- Nausea
- Vomiting
- Constipation.
- Tummy ache.
- Bug.
- Abdominal Pain
- Diarrhoea
- Changes in bowel movement.
What are the two systems of medical knowledge?
- Scientific medicine
- Everyday (lay or popular) medicine.
In the 21st century there is an expectation that people use lay referral networks and self-care e.g. NHS choices. What are the advantages and disadvantages of using this system?
Advantages: reduces pressure on GPs and reduces costs.
Disadvantages; may delay diagnosis and treatment.
What are the benefits of complimentary and alternaitve medicine? (CAM)
- CAMs focus on health, wellness and wellbeing.
- CAMs emphasise subjective experience of the whole person: unity of mind/body/spirit.
- CAMs are less hierachical than medicine, which focuses on science and the expert.
- CAMs are ‘natural’ ‘safer’ ‘non-invasive’
CAMs are often less costly.
- They are difficult to test through randomised control trials. In spite of this, 1 in 4 UK reisdents use CAMs.
CAM professions are subject to statutory regulation.
