Esophagus Anatomy
- what makes up the cranial sphincter?
- what is the differnce between dogs and cats?
The oesophagus is a tubular structure connecting the pharynx to the stomach, and is bound at each end by a sphincter. The cranial sphincter is composed of the paired thyropharyngeal and cricopharyngeal muscles.
The caudal sphincter is complex and comprises the following:
- Focal thickening of the muscular part of the oesophageal wall
- Interdigitating gastric rugal folds
- A sling formed by the deep oblique smooth muscle of the lesser gastric curvature and the right diaphragmatic crus
- The acute angle of entrance into the gastro- oesophageal junction
- Positive intra-abdominal pressure compressing the intra-abdominal section of the oesophagus.
The oesophageal wall is composed of four layers: mucosa, submucosa, muscularis and serosa. The muscularis is a striated muscle in the dog, but in the cat the caudal third is a smooth muscle with the overlying mucosa having characteristic herringbone- like folds.
The different muscular anatomy of the canine and feline oesophagus creates specific appear- ances following contrast medium administration . The canine oesophagus has a longitudinal linear pattern on positive contrast studies (Figure 9.4). In the cat the smooth muscle of the terminal third of the oesophagus creates a striated herringbone appearance.
Causes of Megaesophahus
Neuromuscular disorders:
- Idiopathic
- Myaesthenia gravis
- Systemic lupus erythematosis Polymyositis/myopathy
- Glycogen storage disease (type 2) Dermatomyositis
- Distemper virus
- Tetanus
Esophageal obstrution:
- Neoplasia
- Foreign body Stricture
- Vascular ring anomaly
Toxicity:
- Lead
- Organophosphate
Other:
- Hypoadrenocorticism
- Hiatal hernia
- Gastric dilatation-volvulus syndrome
- Oesophagitis
- Thymoma
Esophageal Diverticulum
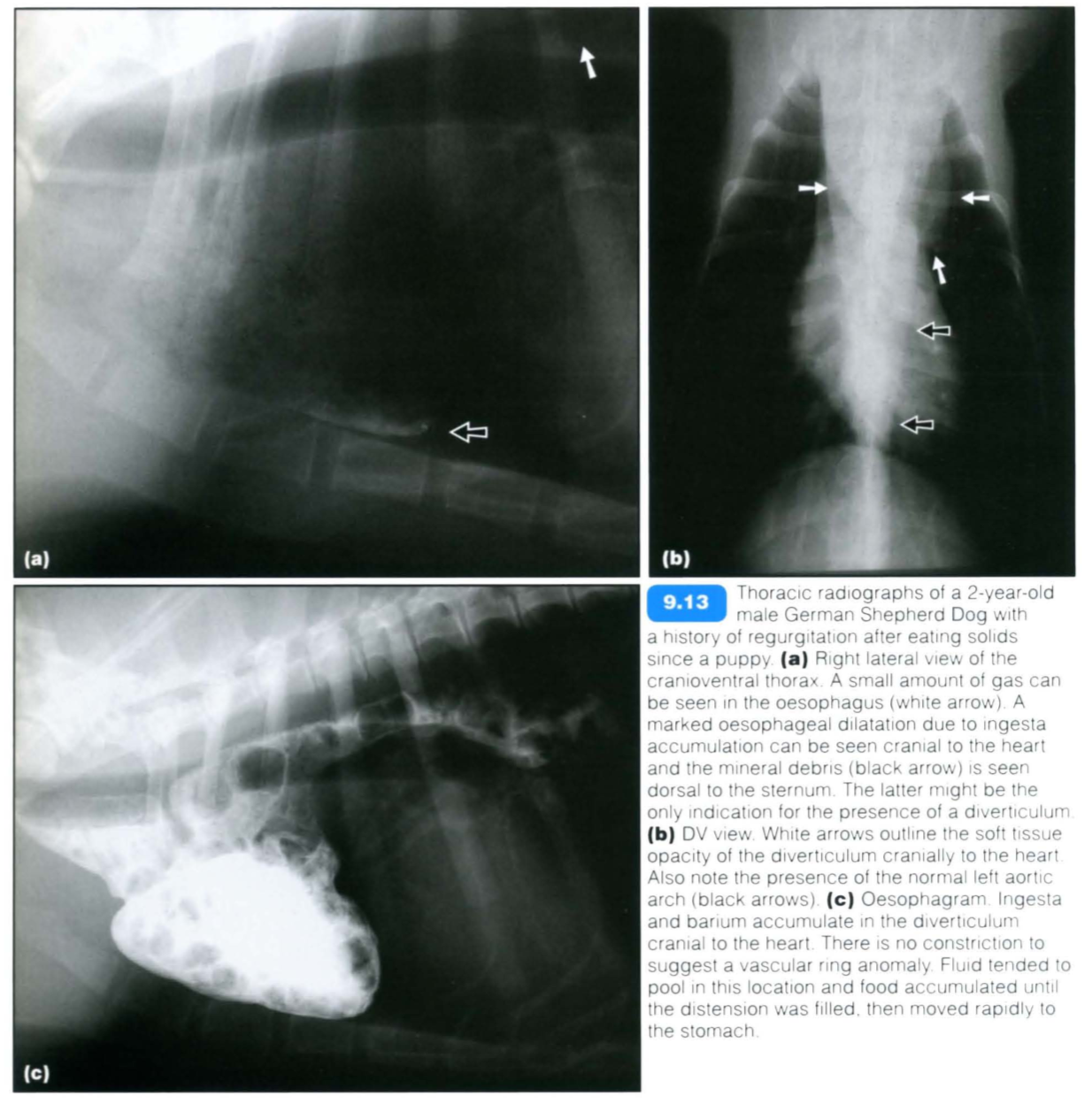
Oesophageal diverticula are rare pouch-like sacculations of the oesophageal wall that may be congenital (Figure 9.13) or acquired. Congenital diverticula occur most often in medium-sized to small-breed dogs. Clinical signs of diverticula are related to the underlying oesophageal disease or to local food stasis and inflammation.
Two types of acquired “diverticula may occur:
- Pulsion diverticula result from conditions of increased intraluminal pressure, secondary to obstruction (stricture or foreign body) or altered motility. The oesophageal wall thins and weakens and bulges out unoer increased intraluminal pressure
- Traction diverticula result from traction on the oesophageal wall, secondary to perioesophageal inflammation, fibrosis and adhesions. These are often small and insignificant.
The accumulation of ingesta within the diverticulum leads to oesophagitis, mechanical obstruction (seen with large diverticula) and disturbed oesophageal motility. Severe cases with mucosal ulceration may eventually perforate, resulting in mediastinitis.
Diverticula should not be confused with a normal redundant oesophagus. Extending the patient’s neck should result in the disappearance of a ‘false diverticulum.
Radiography:
- This is usually normal
- Pouch-like sacculation of oesophagus (gas/ ingesta)
- Ingesta more commonly collects in pulsion than in traction diverticula.
Contrast studies:
- Contrast medium within pouch-like sacculations of oesophagus
- Large multiloculated diverticula may only partially fill with contrast medium
- Pulsion diverticula usually have rounded or multilobed borders, thin wall and neck similar in size to the diverticulum itself
- Traction diverticula usually have triangular shape with wide base at the oesophagus, thick wall and tip pointing to the area of adhesion.
Esophageal Neoplasia
Fibrosarcoma and osteosarcoma developing from malignant transformation of Spirocerca lupi granulomas (see below) are the most common malignant oesophageal neoplasms in dogs. Other oesophageal neoplasms are extremely rare and constitute less than 0.5% of all cancers in the dog and cat. These may be of primary oesophageal, perioesophageal (lymph nodes, thyroid, thymus and heart base; see Chapter 8) or metastatic (thyroid, pulmonary and gastric carcinomas) origin.
Primary neoplasms include:
- Leiomyoma
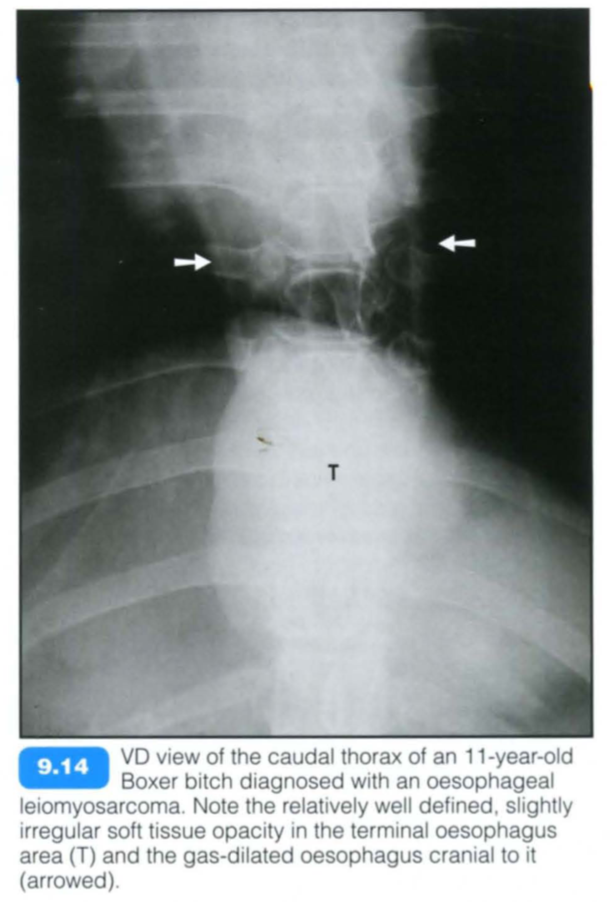
- Leiomyosarcoma
- Carcinoma
- Chondrosarcoma
- Squamous cell carcinoma being the most common in the cat.
Leiomyomas show a slow growth rate and lack of invasiveness, and on occasion may only be recognized at necropsy.
Radiographic findings include:
- Mineralization of oesophageal mass (rare; differentials such as mineralization of a radiolucent foreign body, dystrophic mineralization, accumulation of mineralized food material, coating of abnormal mucosa by radiopaque oral medication should also be considered)
- Soft tissue ‘stripe’ between the descending aorta and the CdVC or midline soft tissue opacity bulge on the dorsoventral (DV)/ventrodorsal (VD) view
- Aspiration pneumonia and thoracic metastasis should be checked for.
Contrast studies:
- A positive or negative (pneumooesophagram) contrast medium may be employed. An intraluminal mass/filling defect and/or obstruction with contrast medium pooling cranially will be demonstrated.
Vascular Ring Anamalies
Vascular ring anomalies are congenital malformations of the major arteries of the heart that entrap the intrathoracic oesophagus and cause oesophageal obstruction. The condition is likely to be heritable in German Shepherd Dogs, Irish Setters and Greyhounds. Vascular ring anomalies are uncommon in the cat.
There are several described vascular ring anomalies:
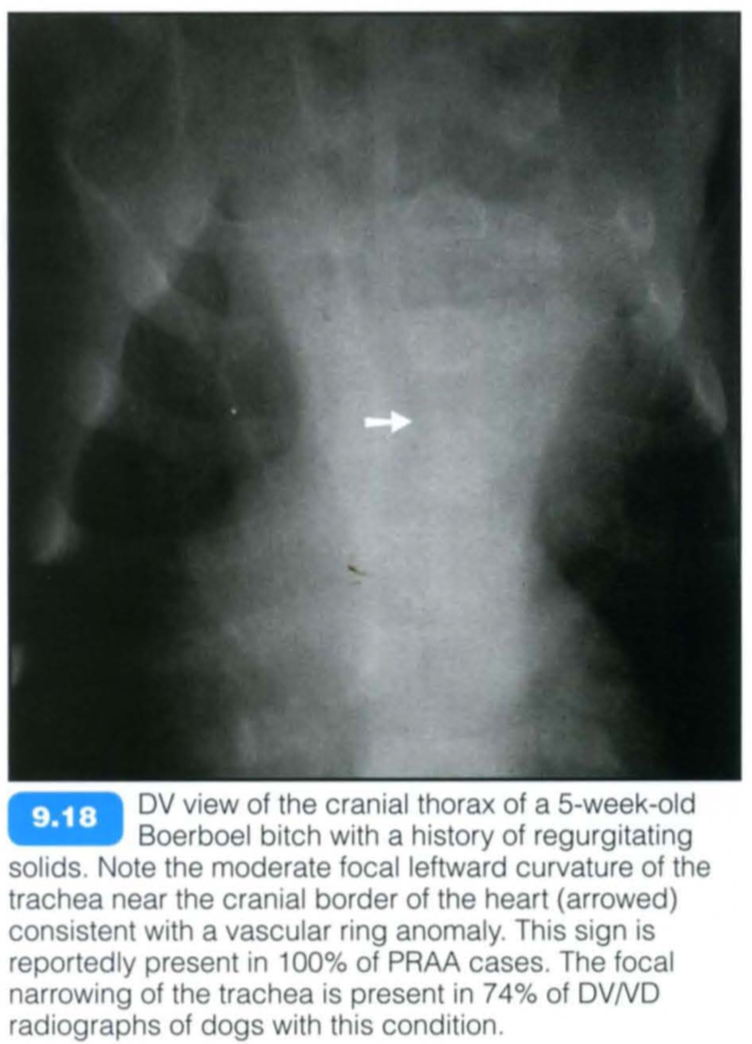
- Persistent right aortic arch (PRAA) is by far the most common (95% of cases)
- Persistent right or left subclavian arteries
- Double aortic arch - may cause dyspnoea
- Persistent right aorta
- Left aortic arch and right ligamentum arteriosum
- Aberrant intercostal arteries
Frequently, additional cardiac or vascular anomalies (such as persistent left cranial vena cava, CrVC) are present but may not be of clinical significance.
Certain clinical signs are similar in all vascular ring anomalies. Most animals present as thin and stunted with a history of regurgitation of solid foods at the time of weaning. Rarely, the ductus arteriosus may remain patent in PRAA (corresponding radiographic signs of patent ductus arteriosus (PDA) should be looked for) and can be auscultated with its characteristic machinery or continuou s murmur. Patients with double aortic arch anomalies may be dyspnoeic due to concomitant entrapment of the trachea.
The prognosis is variable as the oesophageal dilatation and hypomotility are not fully reversible. In general, patients with generalized megaoesophagus or dilatation caudal to the heart have a poor prognosis, and contrast medium administration may be necessary to evaluate this. The earlier the condition is corrected, the better the prognosis.
Radiographic findings include:
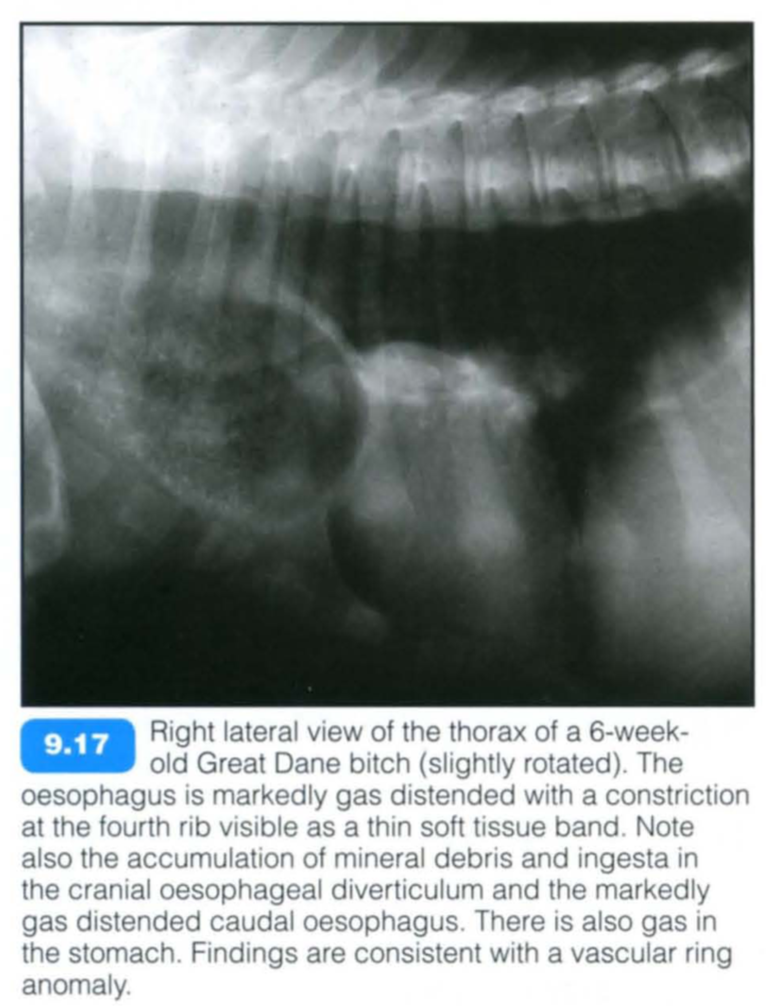
- Oesophageal dilatation or pulsion diverticulum (air/ingesta) cranial to stricture with abrupt tapering at about the fourth intercostal space to the sixth rib
- Ventral deviation of trachea
- Moderate or marked focal leftward curvature of the trachea near the cranial border of the heart in DV/VD radiographs is a reliable sign of PRAA in young dogs with consistent clinical signs. Oesophagography is not necessary to confirm the diagnosis
- Moderate or marked focal narrowing of the trachea
- If a well defined normal left descending aortic margin is visible on the VD/DV view, one of the less common vascular ring anomalies should be considered
- Tracheal stenosis and malformation of tracheal rings are suggestive of double aortic arch anomaly
- Aspiration pneumonia is a common complication of a vascular ring anomaly
- Fibrous bands within the oesophagus may mimic vascular ring anomalies but angiography or oesophagoscopy will confirm the diagnosis.
Contrast studies:
- Contrast medium (barium burger) is recommended for complete evaluation prior to surgery and for prognostic purposes.
- It confirms the location of the oesophageal obstruction and the severity of oesophageal distension.
- The right lateral view demonstrates a curved filling defect associated with PRAA
Spirocercosis
The nematode Spirocerca lupi may lead to the development of oesophageal granulomas and neoplasms. The condition is common in endemic areas (most tropical and subtropical countries) but otherwise very rare. Although any breed can be affected , the condition is seen more commonly in large-breed dogs. Infections in cats are seldom reported.
Eggs containing first-stage infective larvae are eaten by coprophagous dung beetles. Dogs then ingest the beetle or a paratenic host and the larvae penetrate the gastric wall, migrate through arteries and finally reach the thoracic aorta in about 3 weeks. After 10-12 weeks in the aorta the larvae migrate to the oesophagus and it is here that the adult develops within nodules in the oesophageal wall. With time, a granuloma forms and is typically situated in the terminal oesophageal wall. In atypical cases, it may be hilar and smaller. Granulomas may undergo neoplastic transformation to fibrosarcomas/osteosarcomas in 26-41 % of cases. Animals typically present with regurgitation (or less commonly vomiting) or an oesophageal mass may be identified as an incidental finding.
Complications can occur due to perforation of the oesophagus (mediastinitis, pleuritis, mediastinal haematoma, aberrant migration with abscess formation) or rupture of the aortic aneurysm (acute haemothorax) . Parotid salivary gland hypertrophy with hypersalivation may also occur.
Radiographic findings include:
- Midline soft tissue opacity bulge in caudal thorax on DV/VD view. This view is often extremely useful.
- III defined soft tissue opacity in the terminal oesophagus on the lateral view
- Rarely, the mass may be in an atypical location such as the cranial or mid-thoracic oesophagus
- Ventral displacement of the CdVC
- Oesophageal dilatation (gas/ingesta) cranial to the granuloma
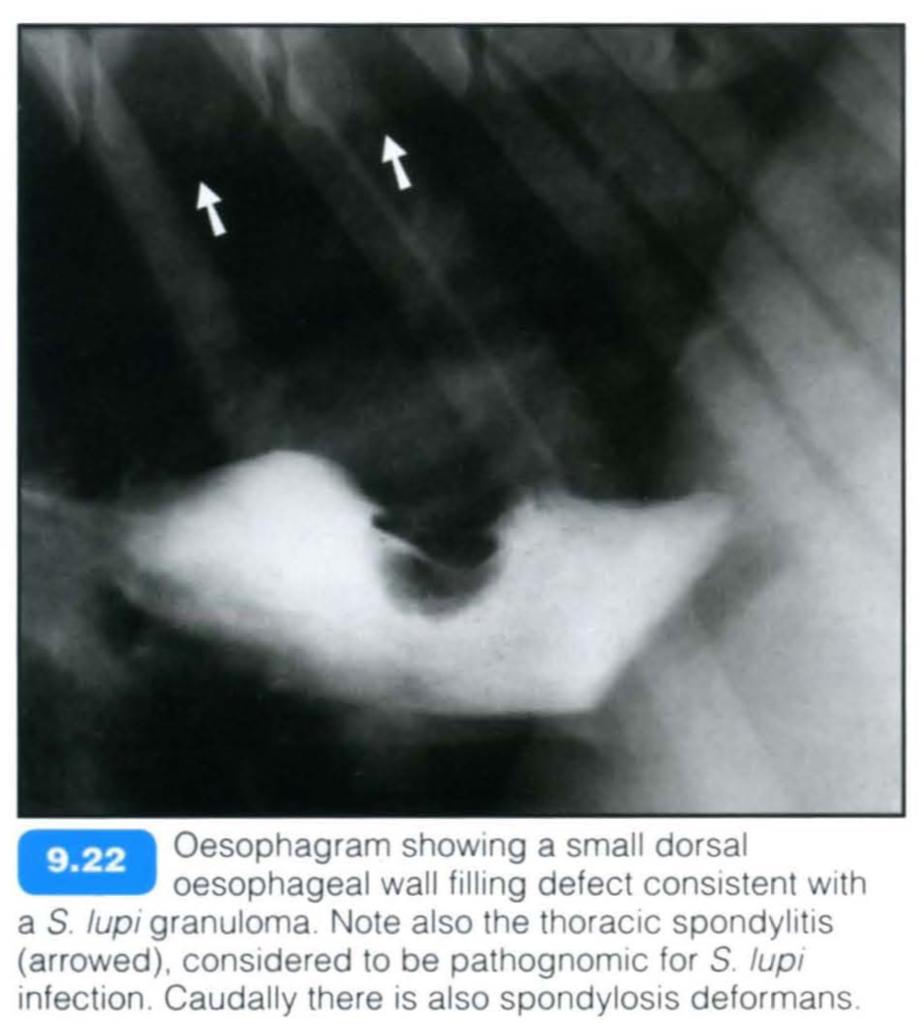
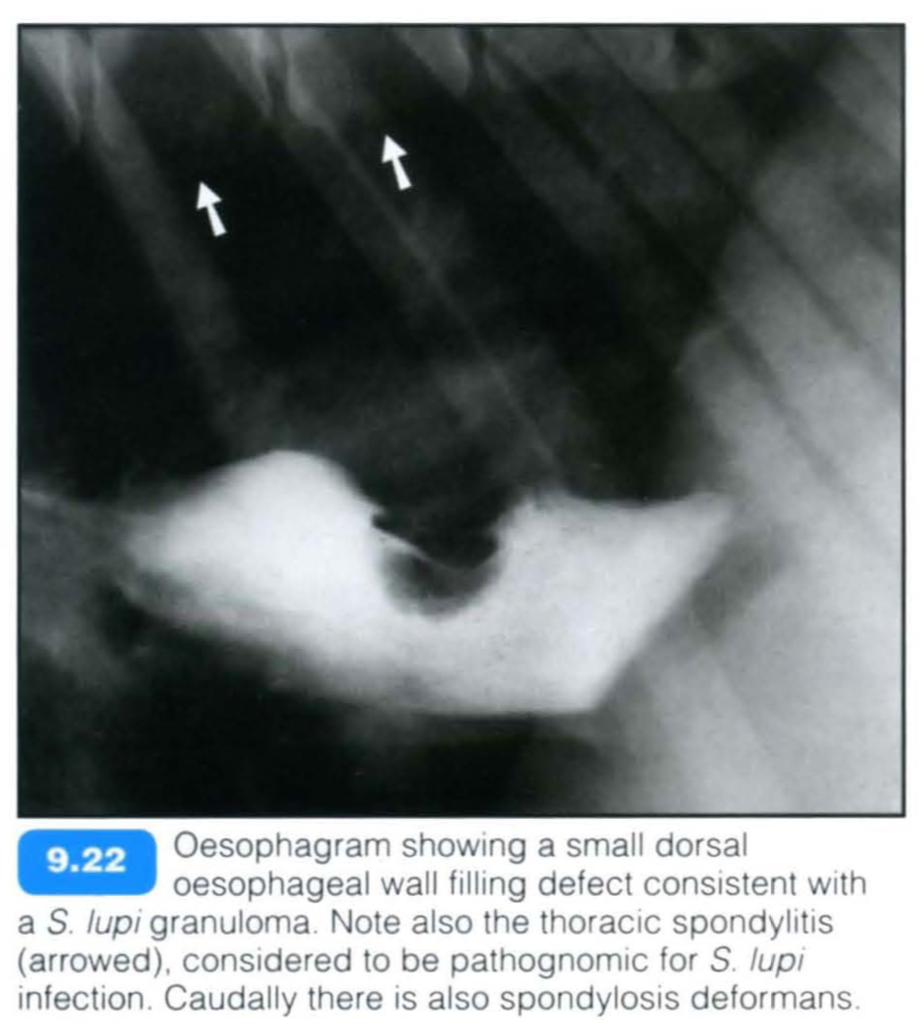
- Spondylitis of last thoracic vertebrae (pathognomonic)
- ‘Pseudospondylosis’ (more lamellar spondylosis, extending to midventral vertebral bodies)
- Mineralized foci within granuloma (trapped mineralized ingesta or metaplasia into osteosarcoma)
- Metastasis to lungs
- Aortic aneurysm
- Hypertrophic osteopathy
- Periosteal reaction on ribs
- Signs of complications
Contrast studies:
- A positive-contrast oesophagram (barium burger is best) or pneumo-oesophagram is used.
- A mural filling defect (often dorsally) is demonstrated
Computed tomography:
- Computed tomography (CT) is recommended when surgery is contemplated for mass resection, It is the most sensitive tool for detection of thoracic metastasis.
- CT is excellent for early detection of focal aortic mineralization and early spondylitis, and therefore extremely helpful in detection of extraoesophageal disease.
- It is best performed with the patient in sternal recumbency, with inflation of the oesophagus with air via the endotracheal tube.
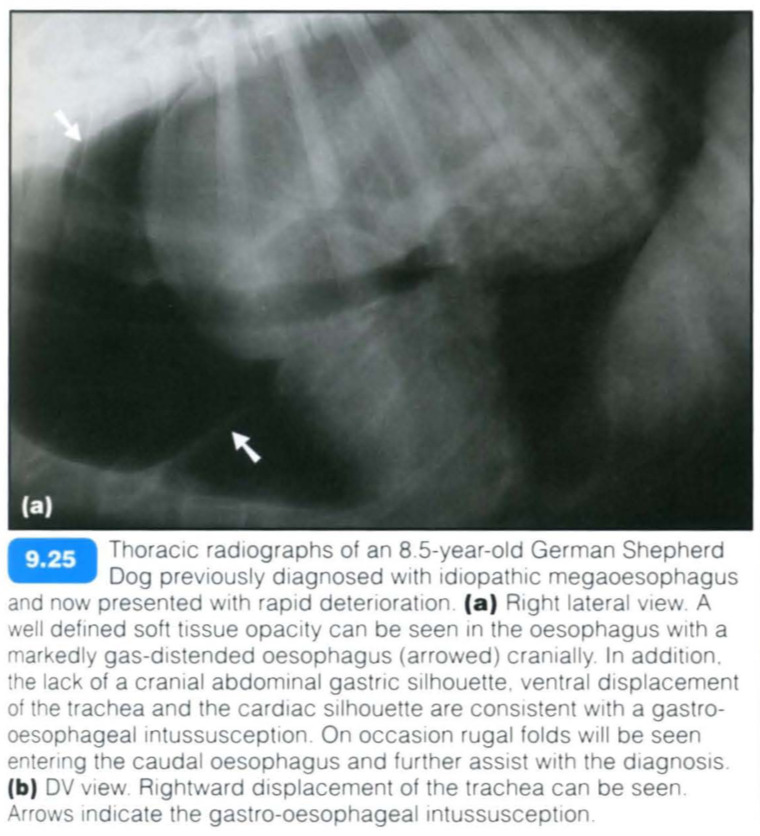
Gastroesophageal intussusception
Gastro-oesophageal intussusception is a condition and results from invagination of the stomach, with or without other abdominal viscera (spleen, duodenum, pancreas and omentum), into the caudal oesophageal lumen.
Predisposing factors include:
- Megaoesophagus
- Congenital oesophageal abnormalities
- Incompetency of the lower oesophageal sphincter
- Chronic vomition
It has been reported to be more common in younger dogs « 3 months. The highest prevalence has been reported in German Shepherd Dogs or large-breed dogs in general.
The clinical signs include regurgitation, vomiting and distress. Rapid deterioration occurs should a large portion of the stomach prolapse into the oesophagus. This constitutes a surgical emergency with mortality rates in excess of 95%.
Occasionally gastro-oesophageal intussusception may be an intermittent problem.
Radiographic findings include:
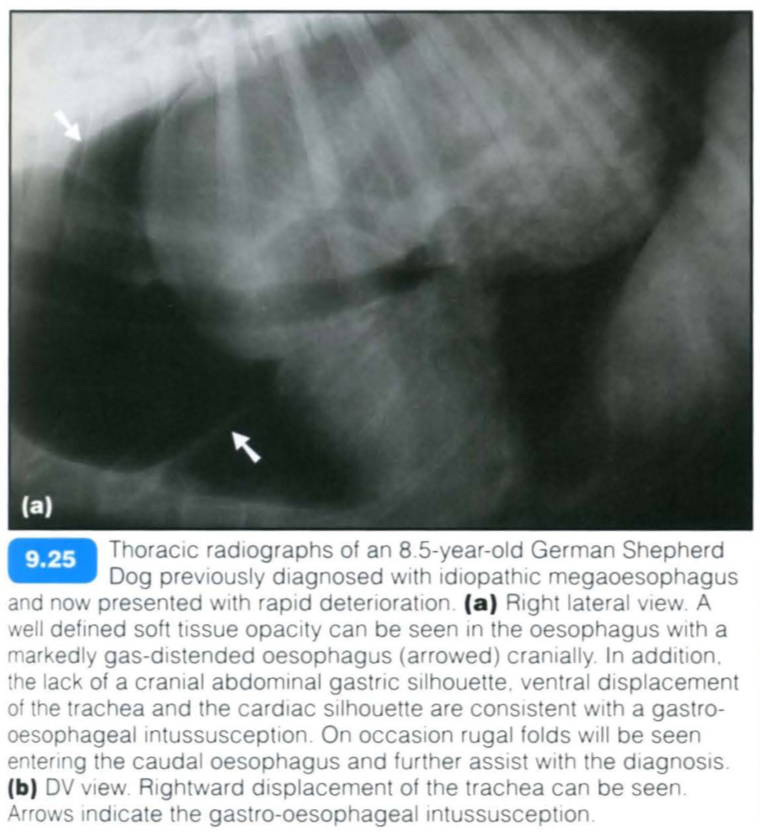
- Well demarcated soft tissue opacity or heterogenous mass within the terminal oesophagus
- Gastric rugae extending into the mass
- Oesophageal dilatation (gas) cranial to the mass
- The gastric silhouette may be absent from the cranial abdomen or when gas-distended its lumen may reveal a defined communication with the mass.
Contrast studies:
- These are contraindicated if surgery is contemplated
- Abrupt cessation of the passage of barium in the oesophagus
- Oesophageal dilatation cranial to the mass
- Gastric rugae within the oesophageal lumen are highlighted
- Contrast medium may outline transverse folds between the dilated oesophageal lumen and the intruded stomach.