Tracheal Hypoplasia
Tracheal hypoplasia is a congenital narrowing of the trachea by at least 50% of the cross-sectional lumen, affecting the entire length of the trachea. The tracheal rings are almost complete with a negligible dorsal muscle.
There is an increased incidence of the condition in English Bulldogs and English Mastiffs, but tracheal hypoplasia has also been described in the Labrador Retriever, German Shepherd Dog, Weimaraner and Basset Hound.
The condition is rarely seen in the cat.
Tracheal hypoplasia is one component of the canine brachycephalic airway obstruction complex, which includes stenotic nares, elongated soft palate and everted laryngeal saccules.
Concurrent congenital abnormalities, such as megaoesophagus and pulmonic and aortic stenosis, have also been identified.
The condition can be diagnosed at an early age, and affected animals may present with stridor, dyspnoea, reduced exercise tolerance and coughing. Excitement exacerbates the condition, which is often progressive during the day. Recurrent respiratory infections may lead to bronchopneumonia .
Dogs and cats with mucopolysaccharidosis VII, a rare genetic lysosomal storage disease causing dysfunctional bone and cartilage formation, can have a similar narrowing of the internal tracheal diameter with thickened misshapen tracheal cartilages.
Imaging findings:
- Radiographically, the trachea appears uniformly narrowed compared with the variation of luminal size along the length of the trachea seen with tracheal collapse.
- Wall thickening may be identified, which can be a result of chronic inflammation or genetic malformation.
- Tracheal growth may be retarded in some animals, which later have a period of compensation, thus the diagnosis should be made with caution in young animals.
The smallest ratio of trachea:thoracic inlet in Bulldogs with no clinical signs of respiratory disease has been established as 0.09.
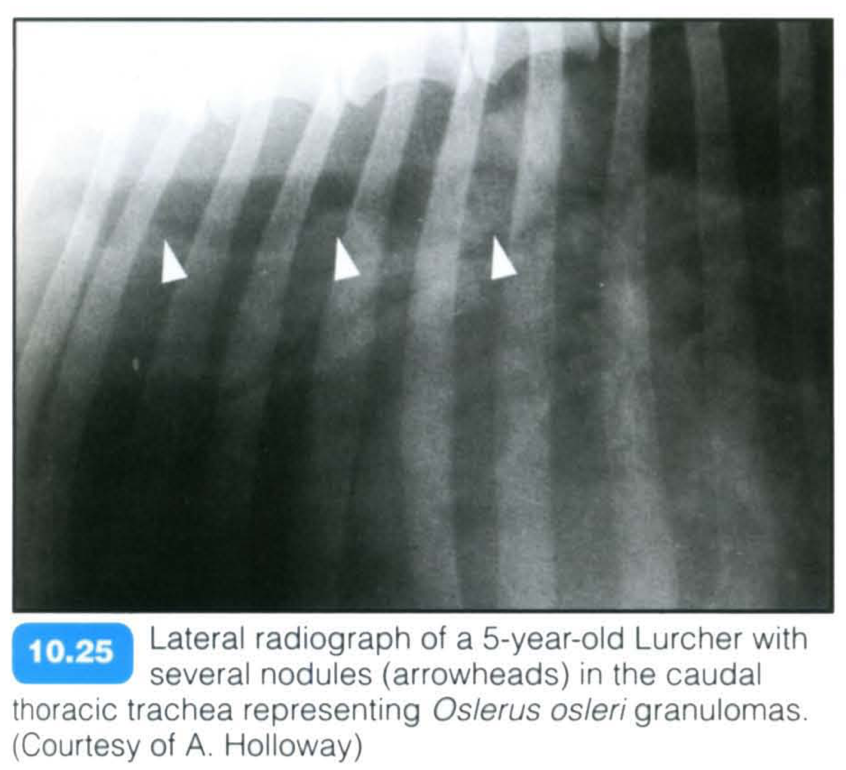
Oslerus osleri infection
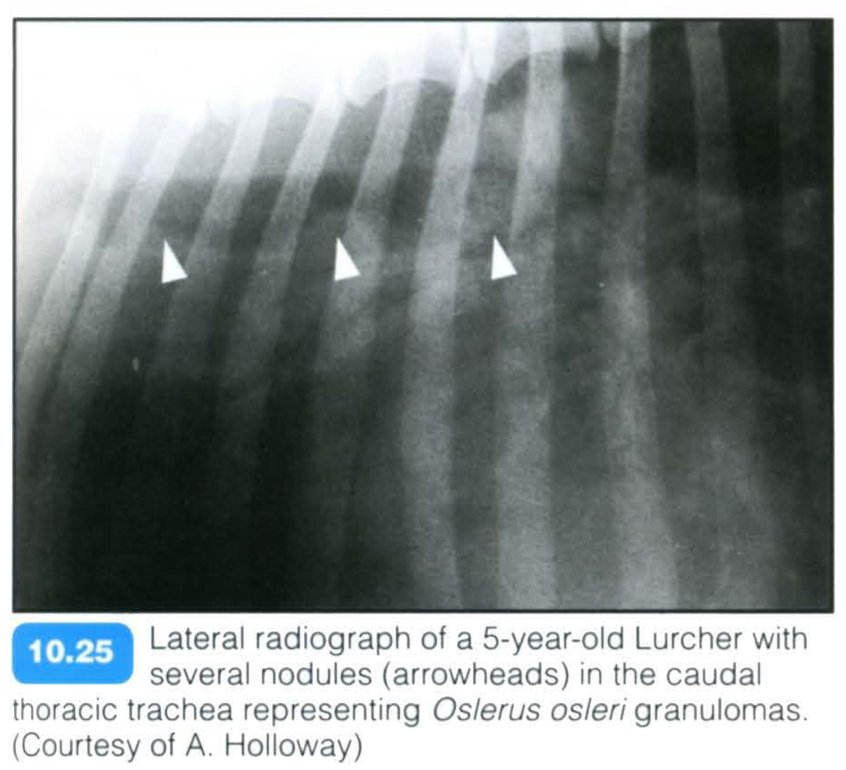
This parasitic infection (previously known as Filaroides osleri) is relatively rare nowadays and is usually identified in dogs less than 2 years old, in particular in kennelled dogs, such as Greyhounds.
Direct transmission from dog to dog is possible, including from dam to pup through faeces and saliva.
Clinical signs include a mild to paroxysmal, hacking and often unproductive cough, which may end in retching, and is unresponsive to antibiotics.
The trachea is sensitive to palpation and, unless a secondary infection is present, a normal body temperature is found.
Wheezing , dyspnoea and weight loss may be seen in more advanced cases, although there may be no clinical signs.
Bronchoscopy is the method of choice for diagnosis, where granulomas, papules or nodules may be identified.
Imaging findings:
- The trachea may appear radiographically normal.
- In severe cases, diffuse tracheal wall thickening, an indistinct mucosal suriace or soft tissue nodules may be seen protruding into the distal third of the tracheal lumen or bronchi.
Ventral Tracheal Deviation

- Neuroendocrine tumors
- Vertebral tumors
Neuroendocrine cells are characterized by their ability to produce and secrete a neuromodulator, transmitter, or hormone. Examples of NETs include carcinoids, gastroenterohepatic tumors (gastrinoma, insulinoma, glucagonoma), pheochromocytoma of the adrenal gland, medullary carcinoma of the thyroid gland, some pituitary tumors, small-cell lung cancer, multiple endocrine neoplasia (MEN types 1 and 2), and tumors of the chemoreceptor organs.

Anatomy of the Bronchial Tree
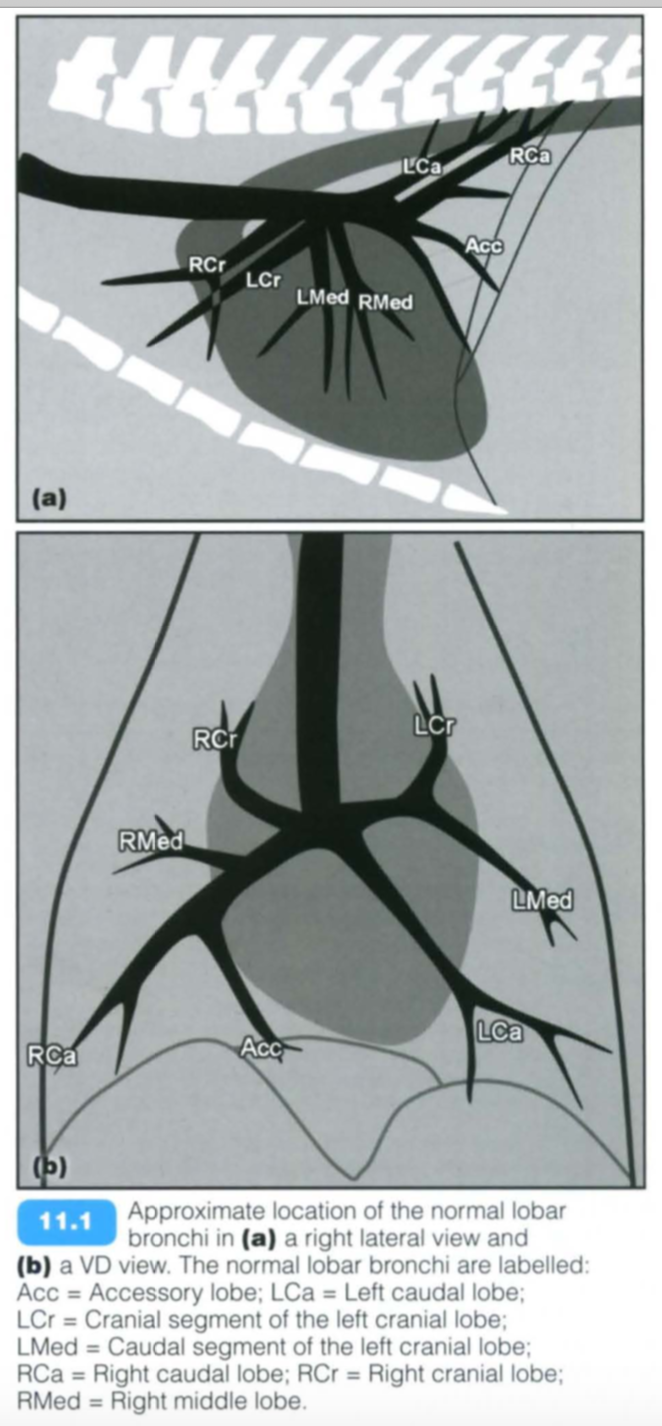
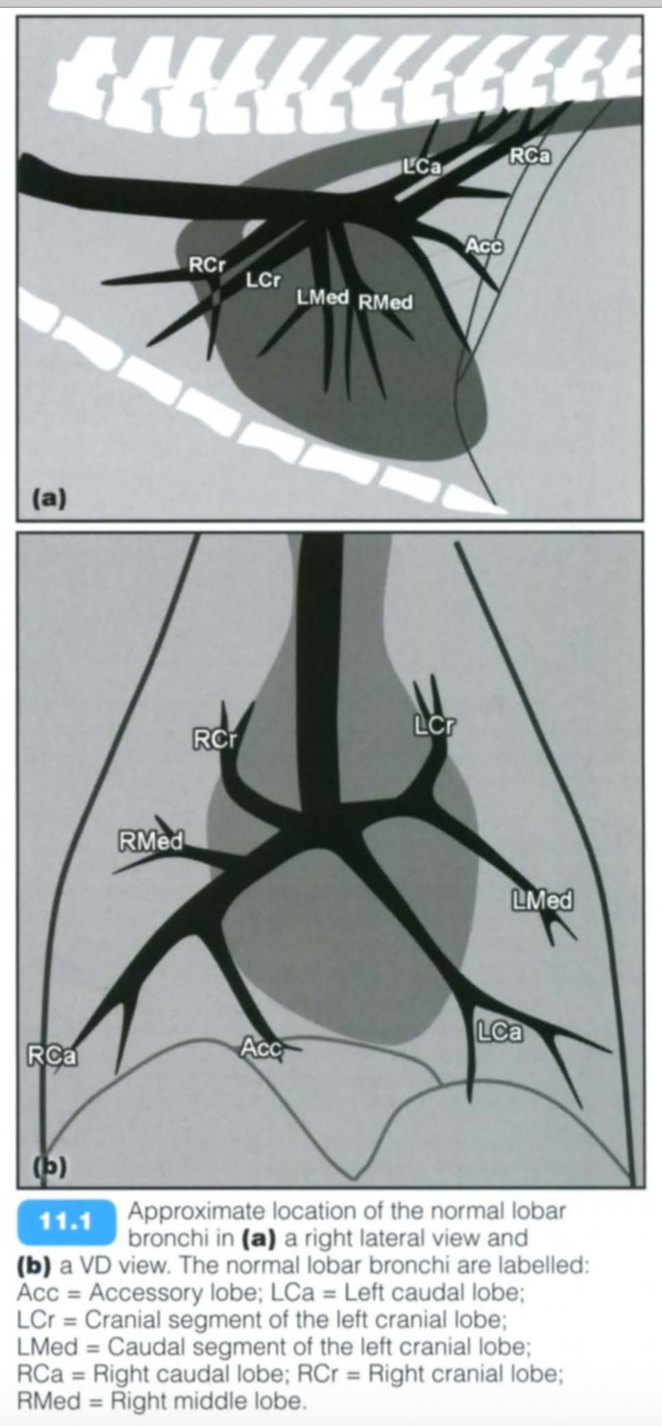
The bronchial tree begins at the termination of the trachea with its division into the right and left principal (or mainstem) bronchi. The principal bronchi are short and each divides into lobar bronchi (also known as secondary bronchi); these supply the various lobes of the lung and are named according to the lobe they supply (Figures 11 .1 and 11 .2).
The right principal bronchus divides into four lobar bronchi. one for each lobe of the right lung:
- Right cranial
- Right middle
- Right caudal
- Accessory
The left principal bronchus divides into two lobar bronchi:
- Left cranial
- Cranial segment
- Caudal segment
- Left caudal
Within each lobe the lobar bronchi subdivide further into segmental bronchi (sometimes referred to as tertiary bronchi). The segmental bronchi with the lung tissue they ventilate are called bronchopulmonary segments. Each bronchopulmonary segment is independent. Adjacent bronchopulmonary segments normally communicate with each other in the dog through the interalveolar pores of Kohn and channels of Lambert (see also Chapter 12). The segmental bronchi branch into smaller generations of bronchi until the formation of the respiratory bronchioles, alveolar ducts, alveolar sacs and pulmonary alveoli. The number of generations depends on the size of the animal and is difficult to measure.
The bronchial walls are formed by hyaline cartilage rings and spiral bands of smooth muscle. Bronchioles are commonly less than 1 mm in diameter and have no cartilaginous support.
Bronchi and the surrounding tissue, up to the level of the respiratory bronchioles, receive their blood supply from the bronchial artery, which, although variable in origin, is commonly a continuation of the bronchoesophageal artery. Venous return is via the pulmonary circulation.
The space between the paired pulmonary artery and vein on a radiograph does not necessarily represent the bronchial lumen. Bronchi should gradually taper towards the periphery
Bronchial Obstruction
(causes)
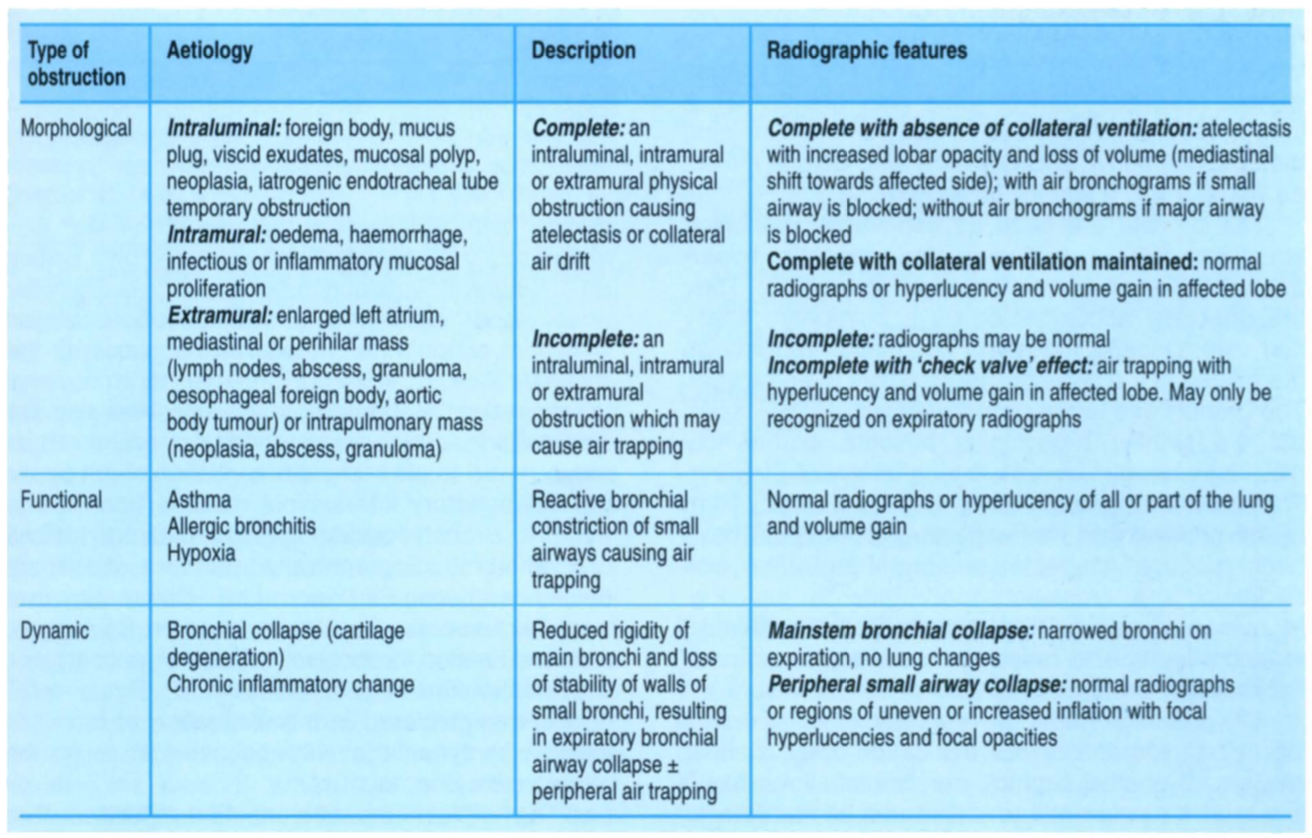
Bronchial obstruction can be produced by a variety of mechanisms. The same classification system can be applied to tracheal obstruction.
- Morphological obstruction:
- A structural obstruction of the bronchus and may be further classified as intraluminal, intramural or extramural, depending on the origin ofthe obstruction.
- Morphological obstructions may be complete or incomplete depending on their size and location.
- Rarely a morphological obstruction (especially a foreign body) can create a ‘check valve’ effect where air is permitted to pass the obstruction during inspiration when the bronchial lumen is wider, but not during expiration when the lumen is narrower. This results in peripheral air trapping and overinflation. This change may not be apparent on inspiratory radiographs but will be identified as a hyperlucent region of lung on expiratory films .
- Functional obstructions:
- Occur when the bronchi constrict with resultant air trapping.
- This may occur in asthma or allergic bronchitis and is discussed further below (see Feline chronic lower airway disease).
- Dynamic obstructions:
- Occur when there is loss of the normal recoil or rigidity of the bronchial walls, resulting in flattening or collapse during forcible expiration or coughing.
- This condition often accompanies tracheal collapse and is discussed in more detail below (see Bronchial collapse).
The radiographic features of bronchial obstruction depend on the location and degree of the obstruction, the effectiveness of collateral ventilation and the chronicity of the condition.
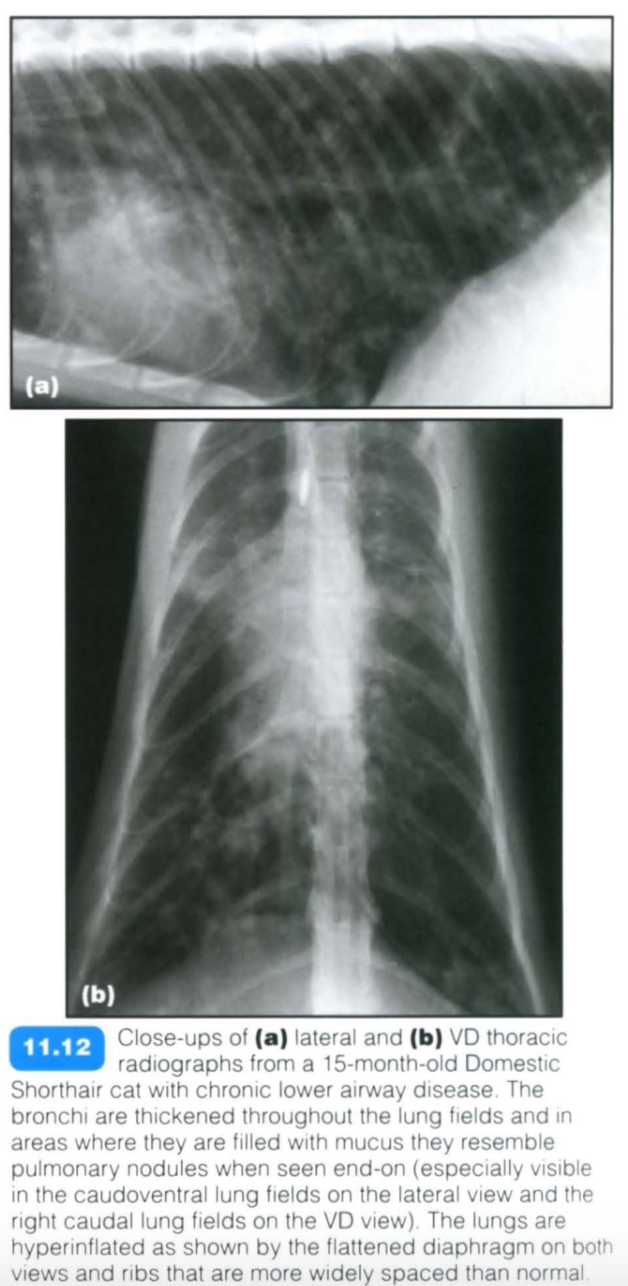
Feline Chronic Lower Airway Dz
Feline chronic lower airway disease
Feline chronic lower airway disease encompasses a multitude of small airway diseases in the cat including feline asthma. Inflammation of the airways leads to a reversible obstruction to airflow (functional obstruction) and hence air trapping. The obstruction is due to a combination of bronchoconstriction, bronchial wall oedema and submucosal gland hypertrophy.
Clinical signs vary from chronic coughing and wheezing to severe respiratory distress. The condition can affect cats of any age with Siamese appearing to have an increased incidence . Hyper-responsive airways and reversible airflow obstruction lead to a reduced airway diameter and increased airway resistance. The condition can be extremely severe in presentation and care should be taken when handling dyspnoeic cats.
Radiography:
- Radiographs may be normal.
- It should be noted that the severity of the radiographic signs may not correlate with the clinical signs.
- Classically peribronchial cuffing is identified, although a variety of bronchial, interstitial and alveolar lung patterns may be observed
- Excessive mucus production and accumulation in the bronchial lumen may give the impression of pulmonary nodules if seen end-on
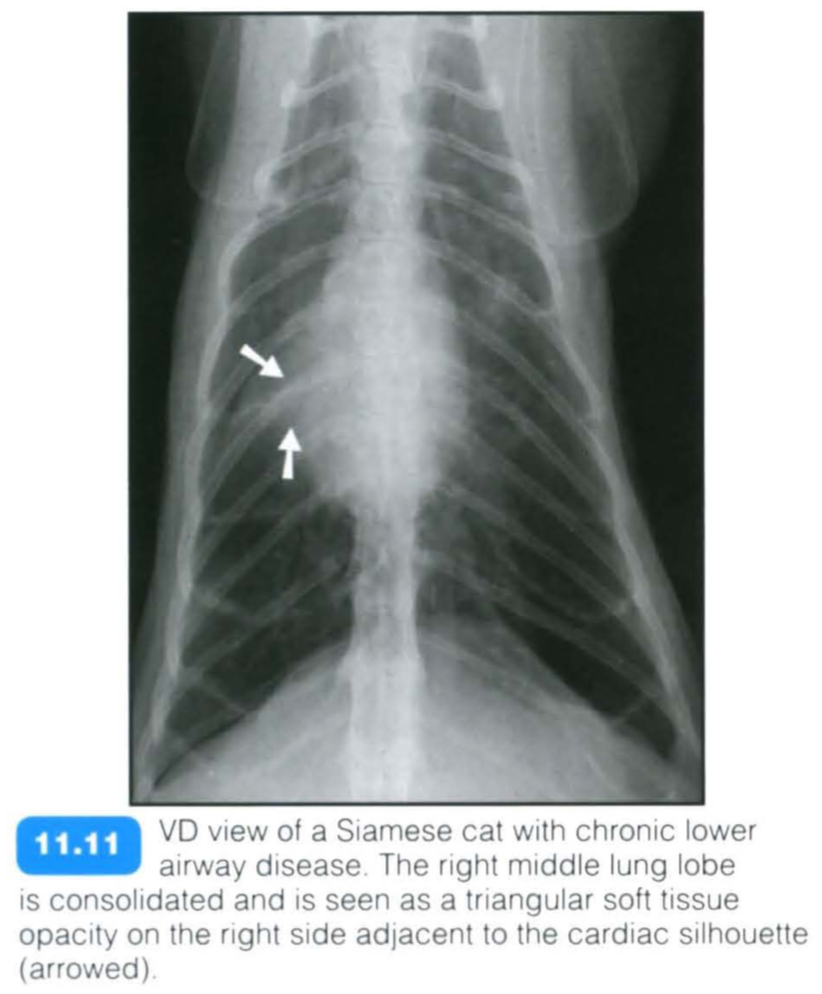
- Obstruction of larger airways can cause alveolar infiltrates, consolidation or atelectasis
- In particular, right middle lung lobe collapse is a common sequel to severe feline chronic lower airway disease
- Evidence of air trapping and hyperinflation may be seen:
- flattened diaphragm
- hyperlucent longs - variable depending on the lung pattern present
- Severe coughing may produce rib fractures in the cat and on occasion multiple fractures at differing stages of healing may be identified
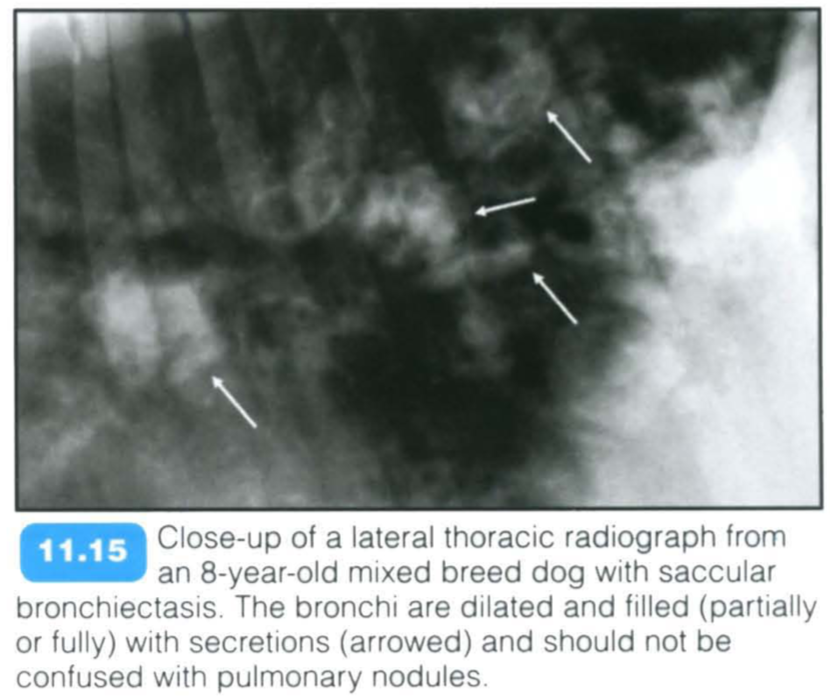
Bronchiectasis
Bronchiectasis is irreversible bronchial dilatation often with accumulation of pulmonary secretions. It can be focal or disseminated and it is uncommon in dogs and rare in cats . In cats, a predisposition for older males has been described.
Causes include:
- A sequel to long-standing infectious or inflammatory pulmonary disease
- Secondary to airway obstruction or smoke inhalation
- As a complication to radiation-induced pneumonitis
- In association with primary ciliary dyskinesia
- It has also been noted that halothane dilates airways by blocking baseline vagal tone.
Bronchial secretions accumulate in the dilated bronchi and predispose the patient to recurrent airway and pulmonary infections.
Dogs with bronchiectasis are commonly presented with a history of chronic productive coughing and recurring pneumonia that initially responds to antibiotics.
Radiography:
- Changes may be localized or generalized
- Widening and unevenness of the bronchial lumen. This may be saccular or (more commonly) cylindrical (also known as tubular) dilatation. Cystic and varicose forms have also been described but are rarely identified.
- Saccular bronchiectases have round drop-like saccules filled with secretions at the end of normal bronchi.
- Cylindrical bronchiectases are dilated bronchi with a fairly even lumen and little diameter change as they subdivide. Each bronchus is club-like and occluded distally
- There may be thickened bronchial walls
- The dilated bronchial lumen may be visualized further into the periphery than normal, e.g. in the ventral areas of the lung fields
- Bronchi filled with secretions/exudate may appear as nodular opacities when seen end-on
- In saccular bronchiectasis many of the bronchi distal to the saccular dilatations are obliterated or filled with an exudate. Occasionally, after secondary infection, the saccules may form localized abscesses
- Often multiple regions of lung consolidation due to accompanying pneumonia
- Development of bronchogenic cysts secondary to bronchiectasis has been described in the dog
- Thoracic radiography may not be sensitive for the diagnosis of bronchiectasis in cats.
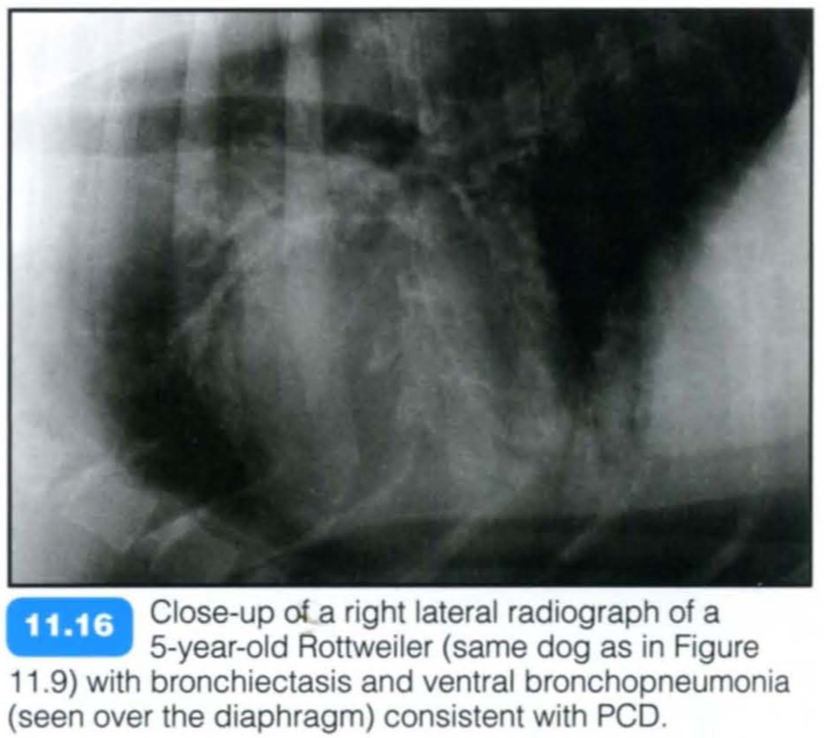
Primary Ciliary Dyskenesia
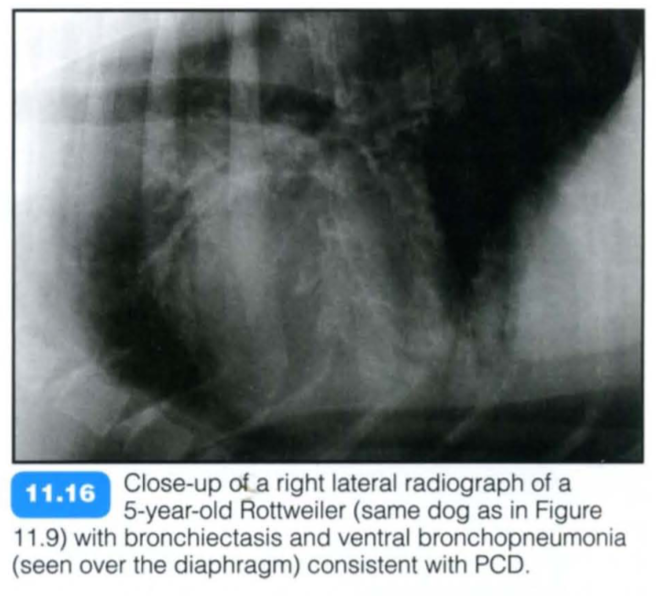
Primary ciliary dyskinesia (PCD), also known as immotile cilia syndrome, is a diverse group of inherited structural and functional abnormalities of the respiratory and other cilia, which results in recurrent respiratory tract infections in the dog. More specifically, PCD is an inherited defect in microtubule formation, affecting cilia of the respiratory and urogenital tract and the auditory canal.
Typically PCD is diagnosed in young purebred animals with a reported higher incidence in the Bichon Frise. The condition may be seen in mixed breed dogs and also in cats.
There is a relatively high prevalence of a respiratory disease and the phenotype is almost identical to PCD in humans. The respiratory manifestations include chronic rhinitis , bronchitis and severe pneumonia with or without bronchiectasis. Affected animals are presented with recurrent chronic nasal discharge, productive cough, respiratory distress and exercise intolerance. Additional findings are infertility, hydrocephalus and loss of hearing.
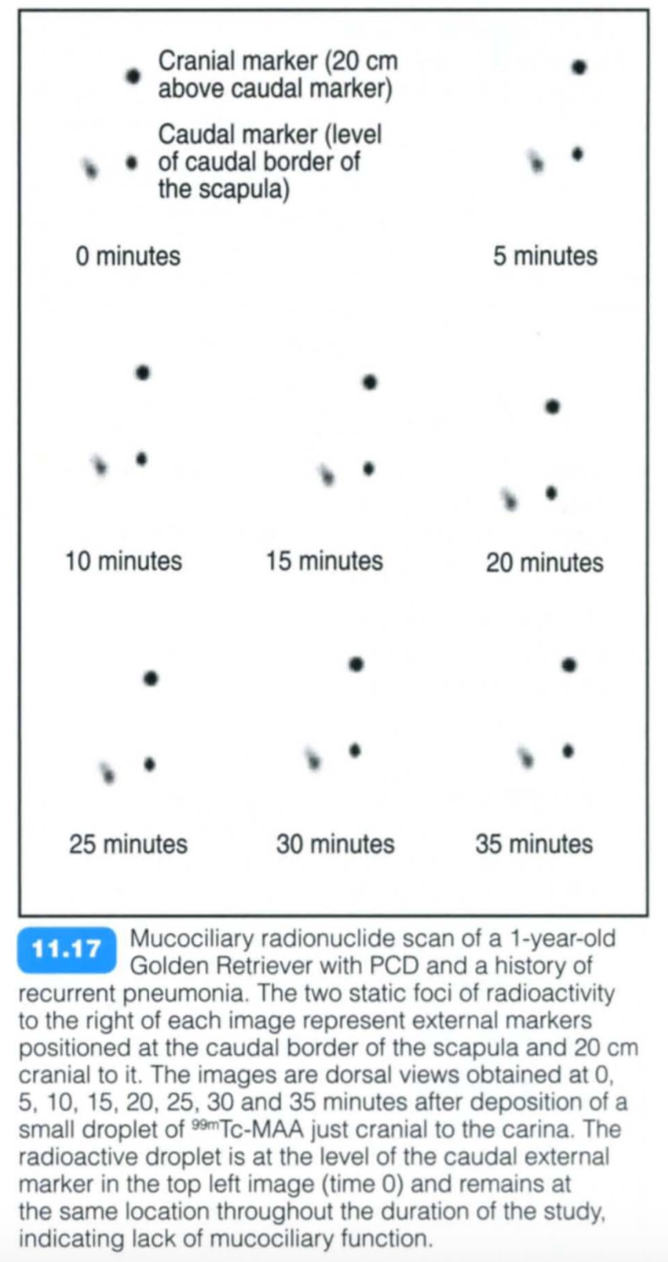
Assessment of deficient mucociliary transport is initially performed with nuclear scintigraphy. Transmission electron microscopy of nasal or bronchial respiratory epithelium or seminal samples provides confirmation of the diagnosis.
Radiography:
- There are variable findings including bronchitis and pneumonia with or without bronchiectasis (Figure 11.16).
Computed tomography:
- Feline PCD has been reported in a 2.5-year-old cat with morphological alterations in the ultrastructure of oviductal cilia. CT findings were consistent with early lesions of bronchiectasis. Foci of pleural thickening and interstitial enlargement were also observed
Scintigraphy:
To perform a scintigraphic study (see Chapter 5) a droplet of 99mTc-MAA is deposited in the distal aspect of the trachea. The diagnosis is confirmed by the absence of movement of the radiopharmaceutical droplet throughout the scintigraphic study. It should be noted that droplet movement always indicates normal Ciliary function (Le. no false- negatives).
Species Differences
- Cranial lung expansion (cranial to the first ribs) is more pronounced in dogs.
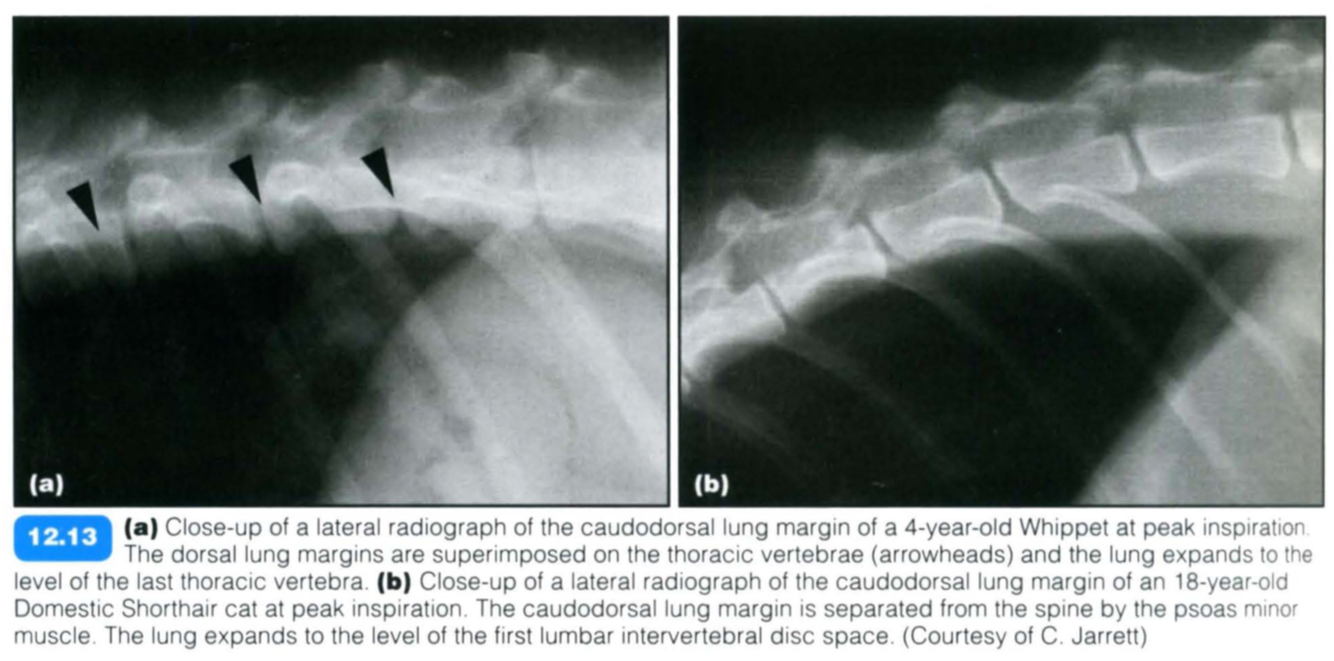
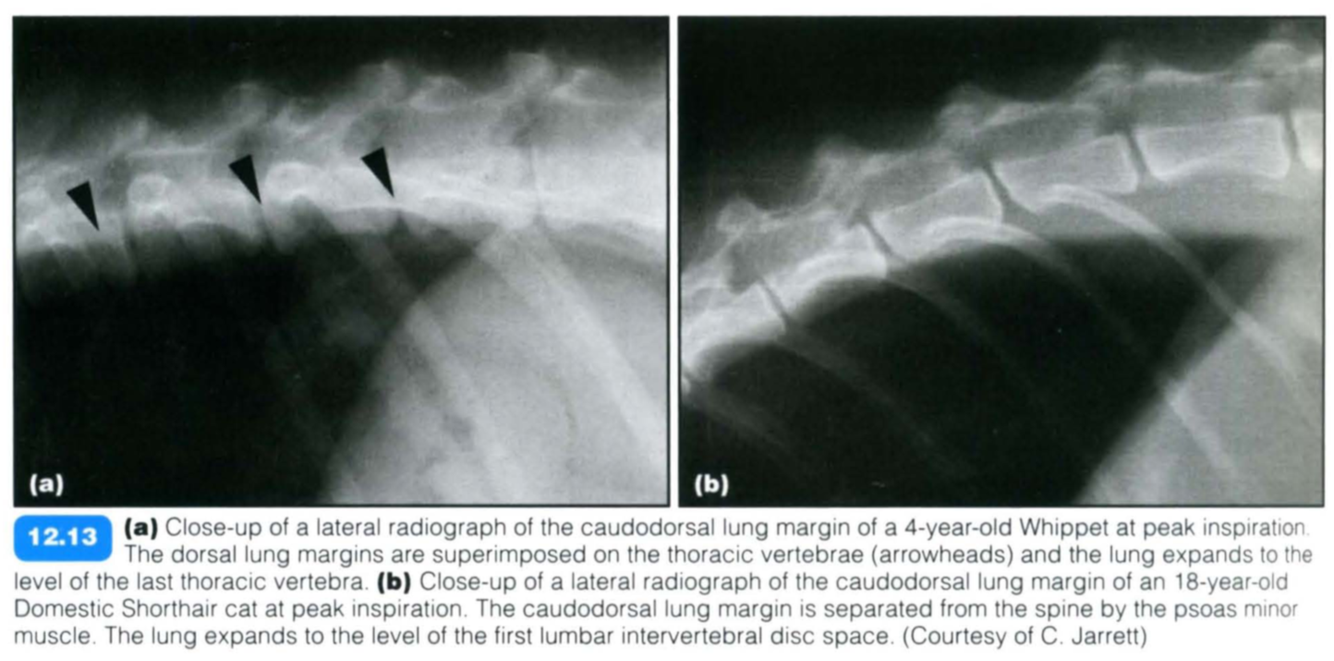
- The feline lung commonly extends further caudally than the canine lung (at peak inspiration to the level of T12-13 in dogs, and L1-2 in cats).
- In dogs, the dorsal lung margins are completely superimposed on the ventral aspect of the thoracolumbar spine. In cats, the caudodorsal lung margin is separated from the spine by the psoas minor muscle, which originates at the ventral surface of the last two thoracic vertebrae (the last thoracic vertebra in the dog).
Obese Animals
Obese animals have large amounts of fat around and within the thoracic cavity, which leads to increased X-ray attenuation and generation of scatter radiation. The net result is an increased lung opacity with poor visibility of the bronchovascular structures. Intrathoracic fat restricts full lung expansion during inspiration, which also contributes to the more opaque appearance of the lungs in these animals. These changes should not be mistaken for pathologically increased lung opacity.
In lean dogs and cats, and in deep-chested dogs, the lungs tend to look very lucent. A close inspection with a highly luminescent light source should reveal normal bronchovascular structures and thereby differentiate this variation from a pneumothorax.
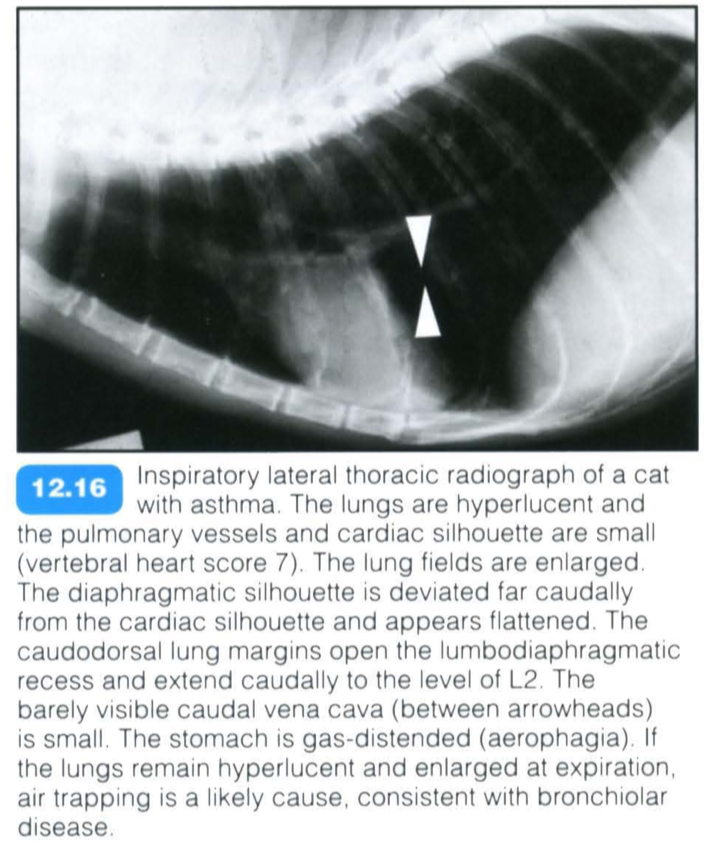
Lung Hyperinflation
Cuases & Radiographic Finidings
Causes:
- Air trapping: one-way valve obstruction of upper or, more commonly, small lower airways. Air can enter the alveoli during inspiration but not leave it during expiration. Seen in patients with:
- allergic small airway disease
- emphysema
- obstructive bronchial masses
- Perfusion deficits: reduced pulmonary perfusion decreases lung opacity and promotes hyperventilation. Seen in patients with:
- right-to-Ieft shunts
- pulmonic stenosis
- right heart failure
- pulmonary thromboembolism
- hypovolaemia
- Central nervous stimulation:
- Stress, commonly seen in hyperthyroid cats, aggressive and feral animals, but also as a normal variant
- Metabolic acidosis
- Shock
- Brainstem pathology (infarct, mass).
General radiographic features include:
- Hyperlucent lung fields:
- Lungs appear darker than normal
- Pulmonary blood vessels appear small but are visible (as opposed to pneumothorax).
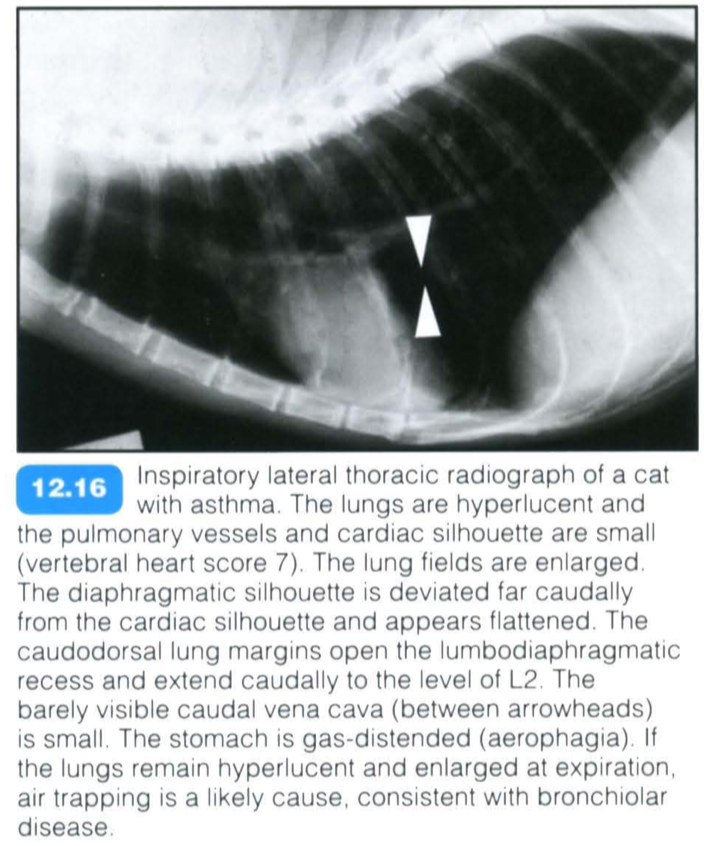
- Enlarged lung fields:
- Caudal displacement of the diaphragm - opening of the costodiaphragmatic recess, resulting in a dome-shaped diaphragmatic silhouette (DV/VD view)
- Opening of the lumbodiaphragmatic recess and flattening of diaphragmatic contour (lateral view)
- Tenting: pronounced visibility of the diaphragmatic attachments to the thoracic wall.
- Small cardiac silhouette and caudal vena cava
- Pleural cupula with cranial lung fields extending cranial to first pair of ribs (in dogs)
- Rib orientation horizontal to the spine on DV/VD view.
- Gas-distended stomach due to concurrent aerophagia .
Pulmonary Metastatic Dz
Radiographic Patterns
- Mesenchymal tumours , which spread primarily via the blood, tend to produce a low number of well defined metastases;
- Whilst epithelial tumours, which spread primarily via the lymphatic system, often produce a large number of relatively small, ill defined nodules. However, this is only a general rule.
Radiographic patterns have been described for several tumour types:
- Haemangiosarcoma: most commonly, poorly defined small coalescing nodules. Less commonly, well circumscribed nodules or an alveolar infiltrate secondary to haemorrhage may be seen
- Transitional cell carcinoma: most commonly, diffuse interstitial pattern or nodular interstitial pattern
- Mammary gland neoplasia in dogs: well defined nodules/ill defined nodules/miliary nodules. Pulmonary alveolar septal metastases is a rare form of mammary tumour metastases described in dogs; the lungs are diffusely infiltrated by carcinoma, predominantly in the arteries and small capillaries of the alveolar septa. It results in a wide range of radiographic manifestations, but most commonly an unstructured interstitial pattern
- Mammary gland neoplasia in cats: ill defined nodules/diffuse pulmonary pattern; less commonly, well defined nodules
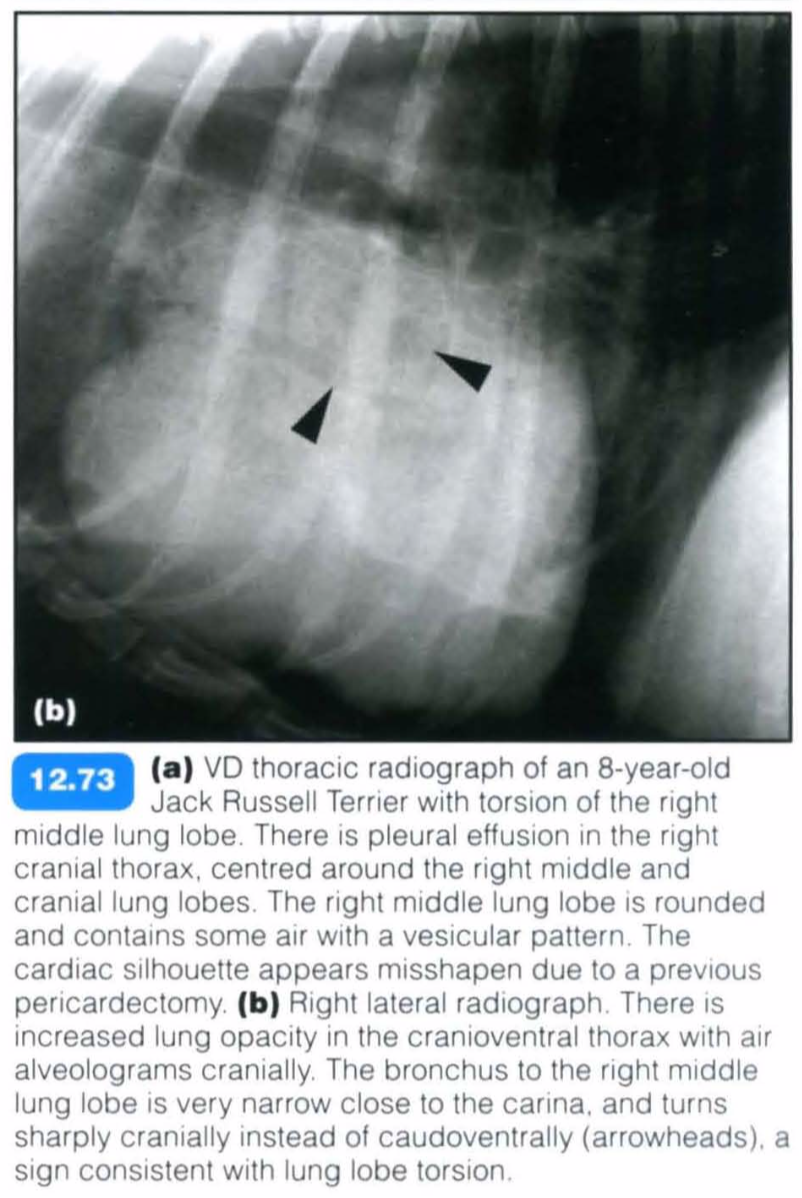
Lung Lobe Torsion

Lung lobe torsion is an uncommon condition in small animals, but it is potentially life-threatening and requires surgical intervention in most cases.
Rotation of a lung lobe occurs around its axis, usually close to the hilus or rarely also in the middle of a lobe:
- This leads to twisting and occlusion of the bronchovascular structures
- Venous return and lymphatic drainage from the lung lobe are compromised, whereas arterial supply is preserved initially to some degree due to the stronger muscular arterial walls
- This leads to venous congestion, pulmonary oedema, sequestration of blood within the twisted lung lobe and eventually lung lobe necrosis
- Blood and fluid enter the alveoli and distal bronchi.
Air can be trapped within the twisted lung lobe due to incomplete bronchial obstruction with a one-way valve effect. Pulmonary emphysema can develop as a consequence of increased alveolar pressure, alveolar or bronchial tears; pneumothorax or pneumo- mediastinum can result from bronchial tears.
Decreased lymphatic drainage, as well as increased interstitial and hydrostatic pressure within the affected lung lobe, leads to production of pleural effusion.
- The effusion initially presents as a transudate.
- It later becomes haemorrhagic or suppurative.
- Necrosis or fibrosis in the later stages of the disease lead to a decrease in lung lobe volume.
Large-breed dogs with deep and narrow chests, particularly Afghan hounds, are predisposed. Small chondrodystrophic dogs with round chests, such as Pugs, have also been described with spontaneous lung lobe torsion. Small dogs and cats are more commonly reported to have an underlying condition, leading to the lung lobe torsion.
Underlying diseases are characterized by collapse of a lung lobe, which is also suspended in either pleural fluid or air, leading to increased lung lobe mobility. Pleural effusion, pneumothorax, trauma with compression of the thoracic cavity and partial collapse of a lung lobe, but also pneumonia and surgical manipulation, are described as predisposing conditions .
The most commonly affected lung lobes are:
- Right middle lung lobe (most common in deep-chested dogs)
- Left cranial lung lobe, the entire lobe or the cranial part (most common in small, chondrodystrophic breeds).
- All other lung lobes can be affected, and more than one lung lobe can be affected. Mid-lobar torsions are possible. Recurring lung lobe torsion has been described, but is unusual.
Radiography:
- Pleural effusion is a consistent finding in patients with lung lobe torsion. The pleural effusion can be :
- Bilaterally symmetrical
- Asymmetrical
- Unilateral and centred around the affected lung lobe
- In most cases pleural effusion is the consequence rather than the cause of the lung lobe torsion, and therefore it may be absent very early on in the disease process. However, this very early stage is rarely observed.
- A mediastinal shift with displacement of the cardiac silhouette is sometimes present, usually away from the affected lung lobe, but can be towards a lung lobe with chronic torsion. The trachea can be dorsally deviated or have some degree of axial rotation at the level of the carina, caused by the abnormal position of the twisted lung lobe. This is best seen on a lateral radiograph.
- Consolidation of the affected lung lobe is evident as an alveolar pattern with loss of visibility of the pulmonary vasculature; whereas, the unaffected lung lobes are relatively normal.
- The affected lobe is enlarged and has rounded borders due to congestion.
- Small air bronchograms or scattered gas lucencies throughout the affected lung lobe (air alveolograms, vesicular gas pattern) result in a foamy appearance of the lung.
- Gas bubbles can also be gathered in ‘clusters’.
- Less commonly, the lung lobe is uniformly opacified without evidence of air bronchograms, as air bronchograms usually disappear after a few days, when the air is replaced by blood or fluid. In chronic cases there is a loss of volume in the twisted lung lobe.
- The lobar bronchus to the affected lung lobe is visible only over a short distance and is blunted, narrowed or ends abruptly close to the carina.
- Air-filled bronchi running in an abnormal direction (inverted air bronchograms) indicate an abnormal position of a lung lobe
- Vessels in an abnormal position are rarely observed due to the consolidation of the lung lobe.
- The adjacent aerated lung lobes are displaced towards the centre of the thorax, evident by a change in direction of the blood vessels and bronchi, as well as the pleural fissure lines.
- Rupture of a bronchus can lead to pneumomediastinum or pneumothorax.
- The change in shape or orientation of the affected lung lobe is best seen after removal of the pleural fluid. In the presence of large amounts of pleural effusion, radiographs should be repeated after drainage of the pleural fluid. In addition, horizontal beam radiographs can provide valuable informatip,1il by shifting the pleural fluid.