Liver anatomy
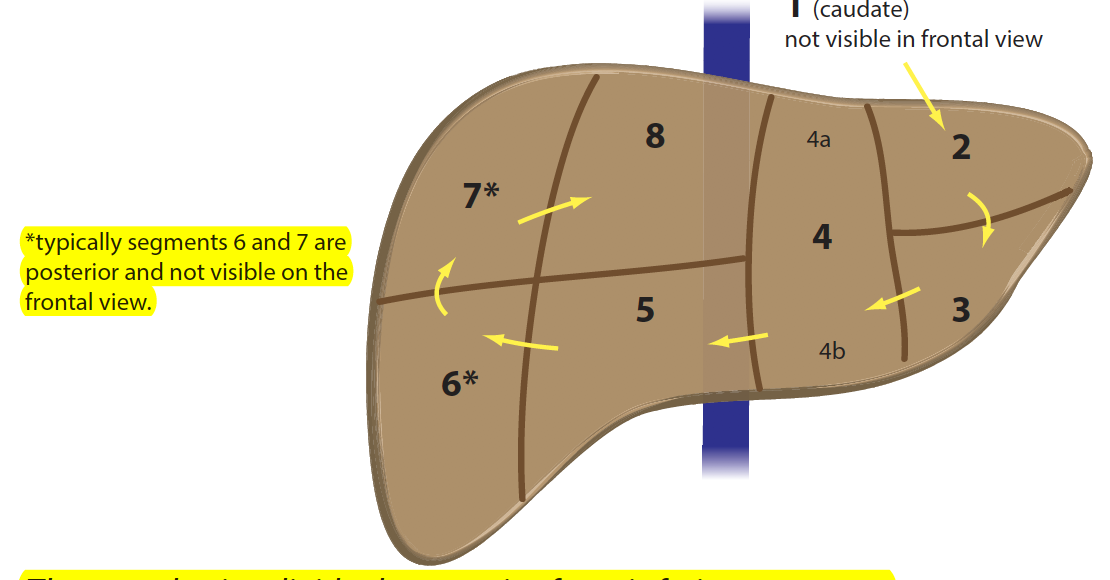
- Segments not typically seen on frontal view.
- % of blood to the liver from where and % w/O2.
- Most common portal vein branching pattern.
- % variant PV patterns.
- 2nd most common PV pattern.
- Where do the hepatic veins run in ech segment?
- 6, 7.
- 75% from portal vein, but provides only 50% of O2.
- Bifurcation into RPV/LPV then RPV bifurcating into RA and RP.
- 25%
- Trifurcation: LPV, RAPV, RPPV.
- Periphery.
- What do the following divide:
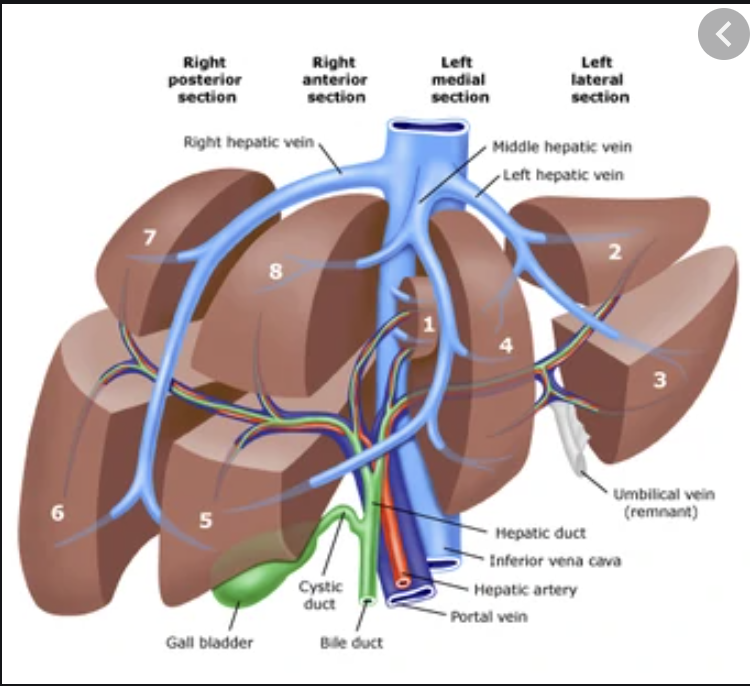
- RHV
- MHV
- LHV/falciform ligament
- Portal vein
- What’s the significance of Cantlie’s line?
- RHV: 7/8, 6/5.
- MHV: 8/4A, 5/4B
- LHV/falciform: 4A/2, 4B/3
- PV: divides upper & lower segments
- Cantlie’s: same division as the MHV.
- Significant as it divides the liver into functional L/R hepatic lobes.
- It runs from the IVC to the middle of the GB fossa.
Liver anatomy: caudate
- Which veins drain this into the IVC?
- Why the caudate hypertrophies in early cirrhosis.
- What other disease causes hypertrophy.
- What is the portal supply to the caudate?
- Veins of Spieghel.
- The caudate may be supplied by R & LPVs. Early in cirrhosis, the caudate is spared of disease from the separate IVC drainage, so the higher pressures don’t affect it as much, then hypertrophies to compensate for crap liver parenchyma.
- Budd-Chiari; direct IVC drainage allows the caudate to bypass the higher HV pressures.
- Branches of BOTH, RPV & LPV supply the caudate.
Liver anatomy: caudate hypertrophy
- DDx (5) & most common.
- How to quantify hypertrophy.
- Cut-off for cirrhosis.
- DDx:
- Cirrhosis: most common
- cavernous transformation of the portal vein
- Budd-Chiari
- PSC (end stage)
- congenital hepatic fibrosis.
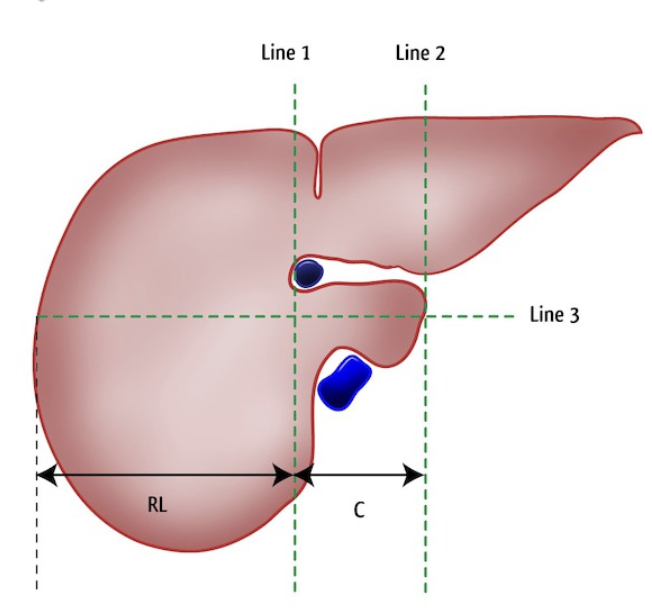
- Caudate-right lobe ratio:
- Take axial slice immediately below MPV bifurcation & draw 3 lines:
- Line 1: R lateral to the PV.
- Line 2: L lateral border of the caudate.
- Line 3: midway b/w the PV & IVC in the caudate.
- Take axial slice immediately below MPV bifurcation & draw 3 lines:
- Caudate-right lobe ratio: >0.65 = high likelihood of cirrhosis.
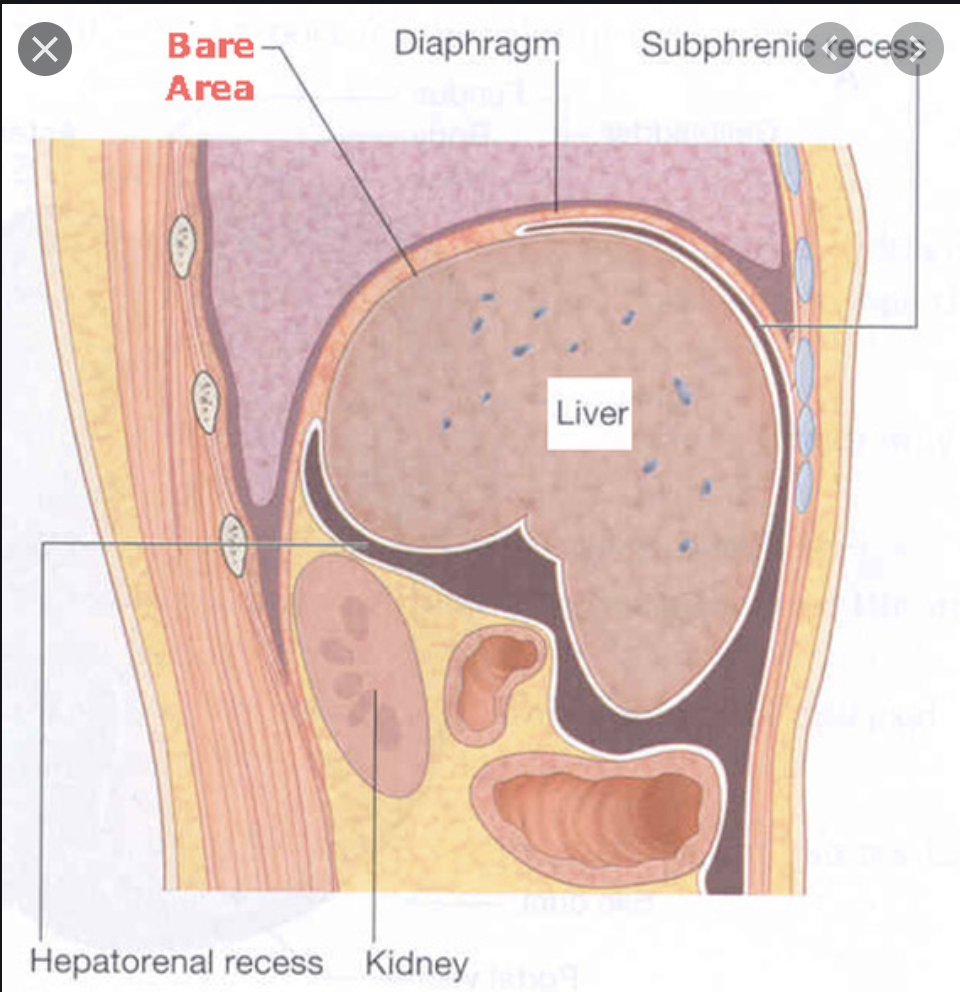
- Name the 3 bare areas of the liver.
- What’s the significance of these?
- Porta hepatis, bare area, GB fossa.
- An injury to the bare area can cause a retroperitoneal bleed.
CT of the liver
- Timing of arterial & PV phase.
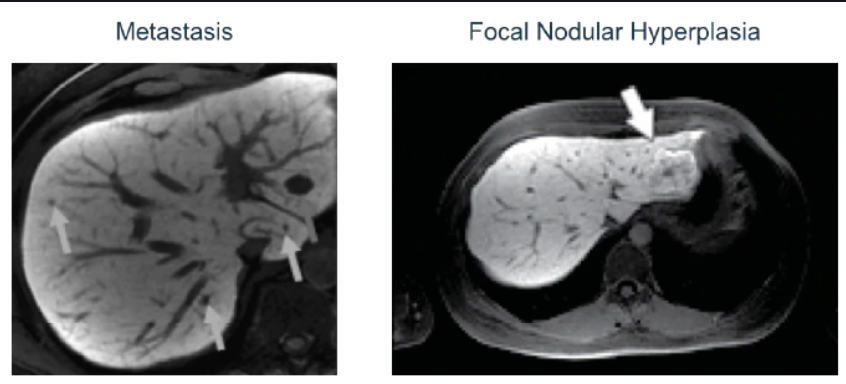
- Vascularity of most hepatic mets. The exception.
- Vascularity of most 1º benign & malignant liver masses. Phase they’re most prominent.
- 25-30 & 70 secs.
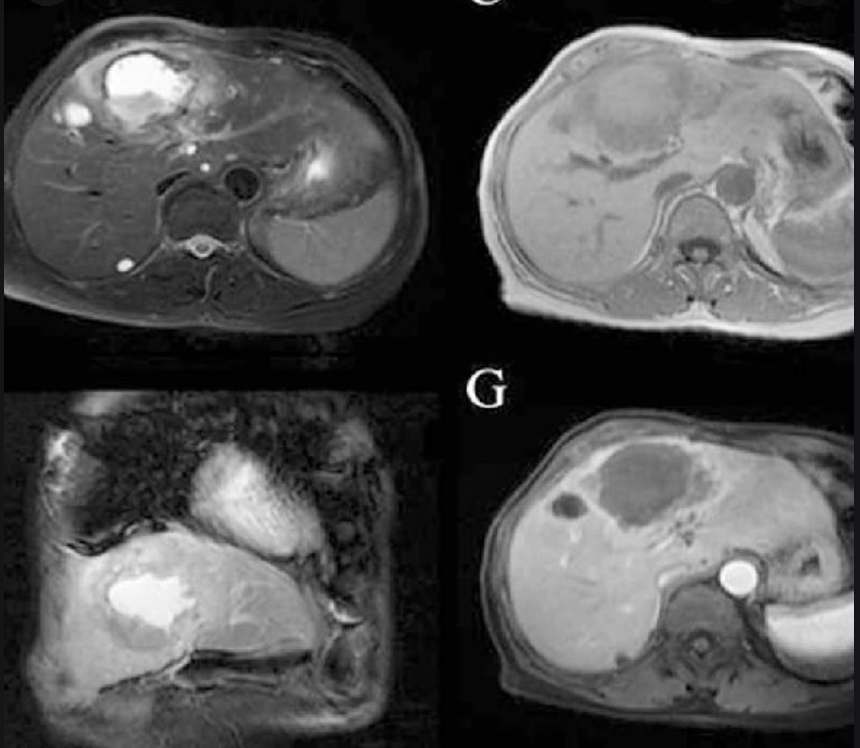
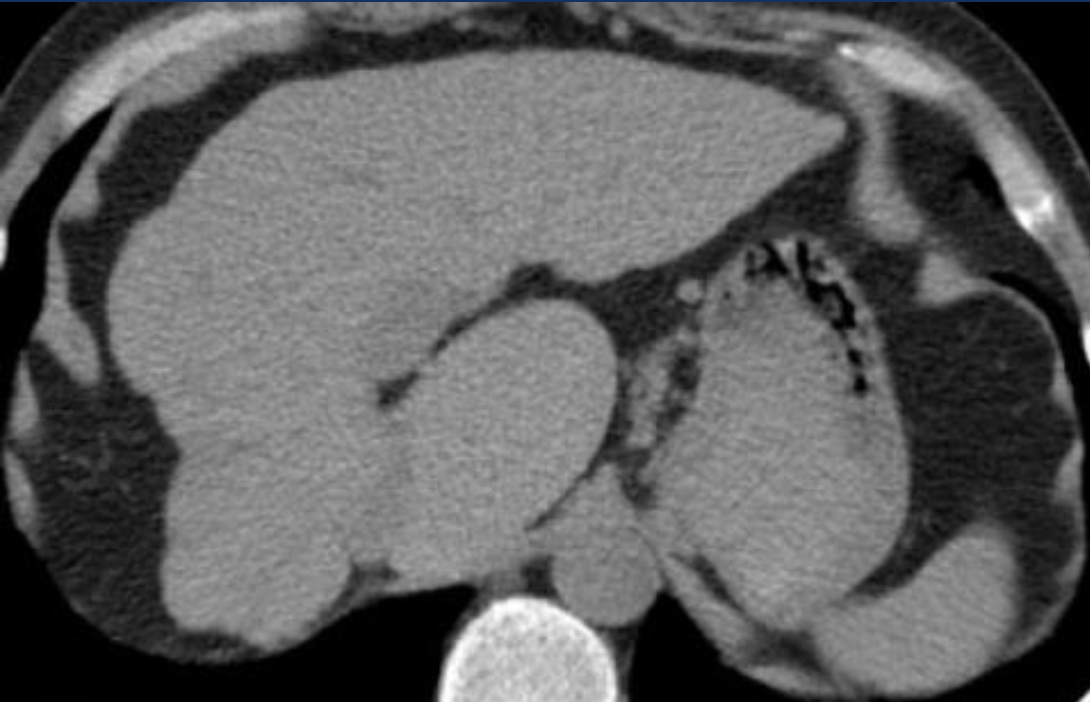
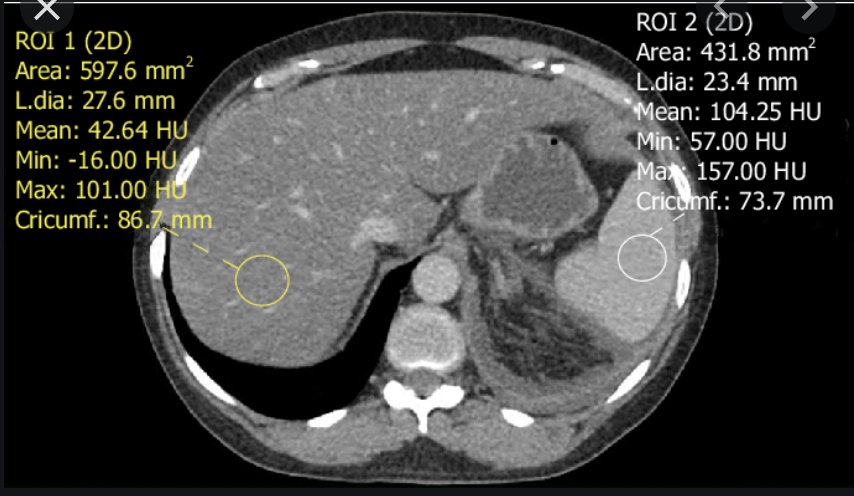
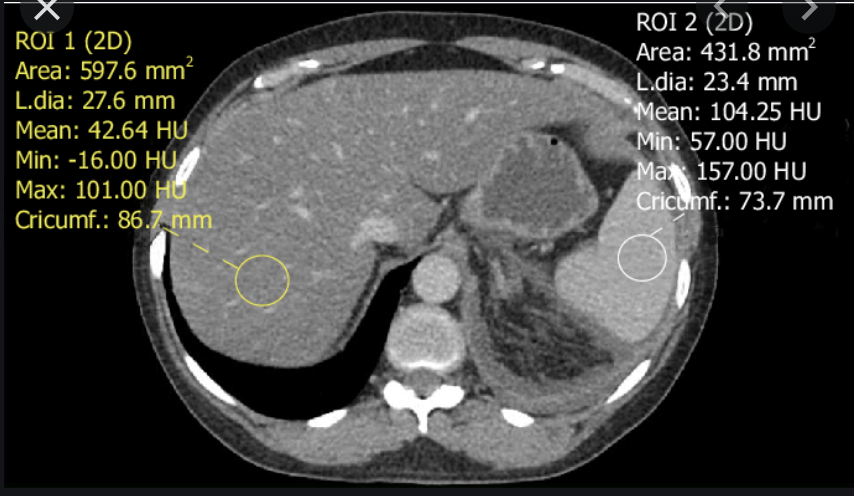
- Mets: hypovascular (see pic). Exception: breast, which can be iso on PV phase & more conspicuous on unenhanced.
- Hypervascular. Most prominent in arterial, typically late arterial (35s).

MRI of the liver:
- Mets/primary enhancement patterns compared to CT.
- Sequences for intracytoplasmic lipid/steatosis.
- 2 types of hepatic MR contrast agents.
- What does Gad do to be bright?
- Same. Mets: hypo; primaries: hyper.
- In/out of phase.
- Extracellular & hepatocyte-specific.
- Shortens T1, just like blood, calcium, melanin, etc.
MR contrast agents: extracellular
- What do these act like?
- Where do they flow?
- Example?
- Purpose?
- CT iodinated contrast.
- Stay outside the cell (extracellular) & are blood flow dependent.
- Magnevist (Gd-DTPA).
- Hepatic lesion detection & characterization; liver vasculature evaluation.
MR contrast agents: hepatocyte-specific
- Where do they flow?
- Examples?
- Is Eovist a pure hep-specific agent?
- When phases are taken
- Purposes?
- 2 other problematic lesions that uptake this?
- Distributes into the vascular then extravascular spaces during arterial, PV & late dynamic phases, then taken up by hepatocytes by the OATP bile uptake transporter into the cell; then excreted into bile.
- Eovist, Primovist.
- No, 55% is excreted into bile.
- MRCP: 5 mins; HPB phase: 20 mins.
- Assess focal liver lesions found on other studies; contrast b/w normal hepatocytes and:
- Great for proving an FNH is an FNH (it uptakes at 20 mins) and not an adenoma.
- Great for finding new mets once all other benign lesions are found: mets don’t uptake.
- HCC surveillance.
- Cholangiogram: bile leaks, GB obstruction.
- FNH, well-differentiated HCC.
Diffuse liver disease: NAFLD
Px: 2 types; components of metabolic syndrome (4).
Ex: prevalence.
Ix: NCCT normal app of liver relative to spleen; HUs.
- NCCT abnormal HU.
- CECT abnormal HU.
- More sensitive test for steatosis.
Px: steatosis, steatosis w/inflammatory activity (steatohepatitis); NAFLD, obesity, insulin resistance, dyslipidemia.
Ex: 15%.
Ix: liver should be slightly hyperattenuating relative to spleen; normal liver 10HU < spleen.
- NCCT: liver >10HU less than spleen.
- CECT: liver >25HU less than spleen in PV phase.
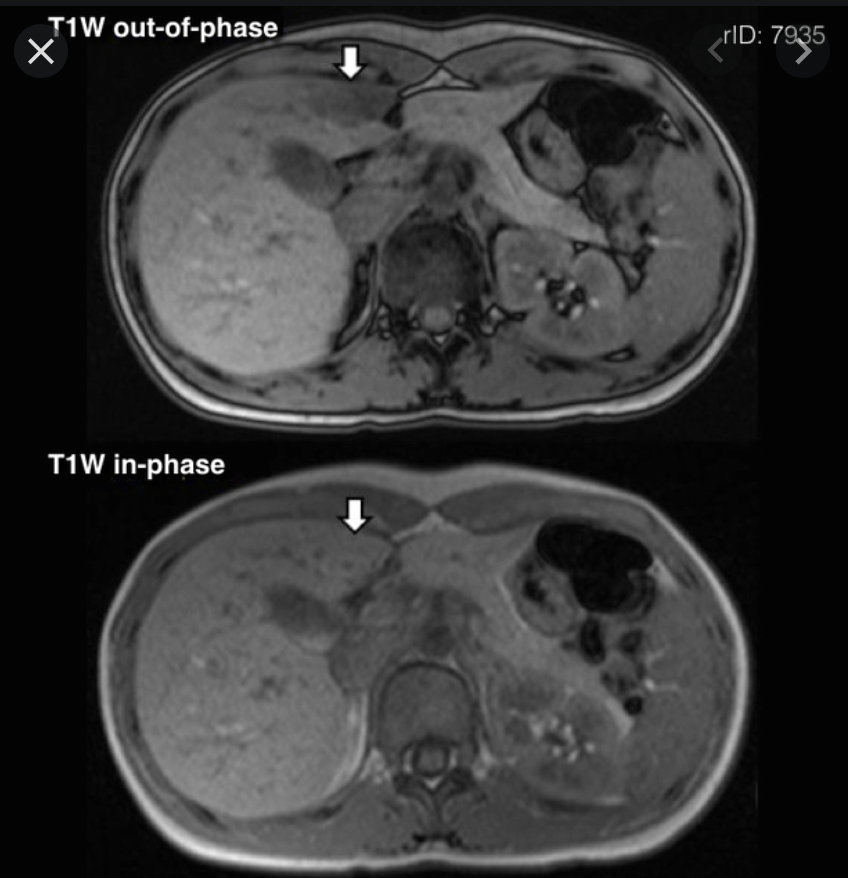
- MR in/out of phase sequences.
DDx hypoattenuating liver (2)
- steatosis: by far the most common
- amyoidosis: rare & may be focal or diffuse
DDx hyperattenuating liver (4)
- Iron overload: by far the most common.
- Medications: amiodarone, gold, methotrexate.
- Copper overload (Wilson’s).
- Glycogen excess.
DDx diffuse/focal hepatic steatosis (5)?
- obesity
- DM
- EtOH
- exogenous steroids
- drugs: amiodarone, methotrexate, chemo
Normal liver attenuation
- Normal NCCT liver range.
- NCCT normal app of liver relative to spleen; HUs.
- Defn hyperattenuating liver.
- NCCT abnormal HU.
- CECT abnormal HU.
- More sensitive test for steatosis.
- Normal NCCT range: 30-60 HU.
- Liver should be slightly hyperattenuating relative to spleen; normal liver 10HU < spleen.
- Hyper: >75HU.
- NCCT: liver >10HU less than spleen.
- CECT: liver >25HU less than spleen in PV phase.
- MR in/out of phase sequences.
Diffuse liver disease: focal fat
Px: why does this form.
- What do the veins of Sappey drain & what can these cause?
Ix: 3 features compared to real masses.
Px: variations in PV supply delivers fat differently, and third inflow (aberrant R gastric venous drainage, veins of Sappey, vein of Burow).
- Sappey: paraumbilical veins draining the ant abdo wall & diaphragm; can cause hot quadrate sign when there is systemic venous obstruction.
Ix:
- No mass effect.
- Vessels run through it, no vessel distortion.
- Characteristic locations:
- GB fossa
- Subcapsular, along the falciform
- Periportal
- Nodular, throughout the liver: hyperechoic on US, hypoattenuating on CT; drop out on OOP GRE.
Diffuse liver disease: NAFLD
Ix: How MR in/out works.
- How this differs from iron overload on in/out.
Ix: when water & fat protons are in the same MR voxel the fat/water signals are summed in in-phase, subtracted in out-of-phase.
- Steatosis: high signal on in-phase, low on out-of-phase.
- Iron overload: low on in-phase, higher on out-of-phase.
Diffuse liver disease: amyloid
Ex: common in liver?
Ix: CT: typical app.
Ex: no, uncommon in liver.
Ix: CT: decreased attenuation, hepatomegaly, “lardaceous liver”.

Diffuse liver disease: Wilson disease
Px: cause; genetics; where else does the deposn occur; most common manifestation in childhood; hepatic sequelae.
Ix: general findings; unique hepatic findings in Wilson’s.
Px: copper accumulation; AR genetic defect; liver, basal ganglia, cornea.
- Most common manifestation: hepatic dysfunction.
- hep sequelae: hepatomegaly + cirrhosis.
Ix: general: hyperattenuation + cirrhosis
- Unique: multiple nodules, perihepatic fat layer + normal caudate.

Diffuse liver disease: hepatic iron overload
- 2 pathways
- Most common
- Pathology of each
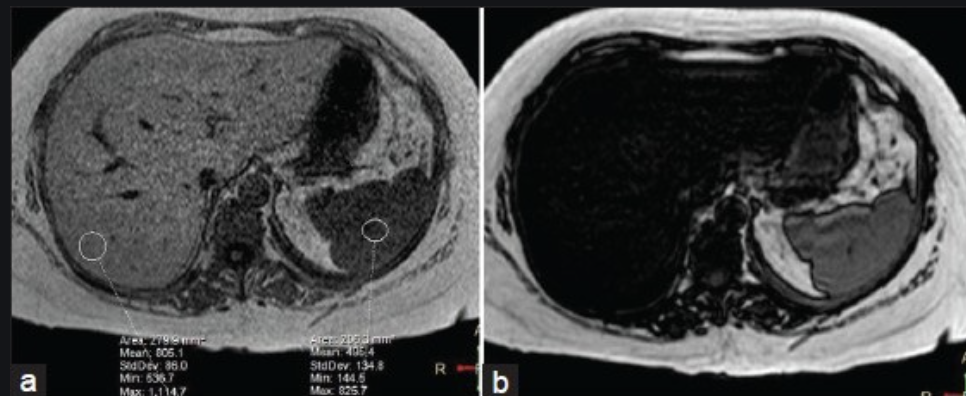
- Ix: general appearance on MR
- Hemochromatosis & hemosiderosis
- Hemochromatosis most common
- Hemochrom: accumulation in hepatocytes.
- Hemosid: accumulation in the RES causes hepatic Kupffer cell iron overload.
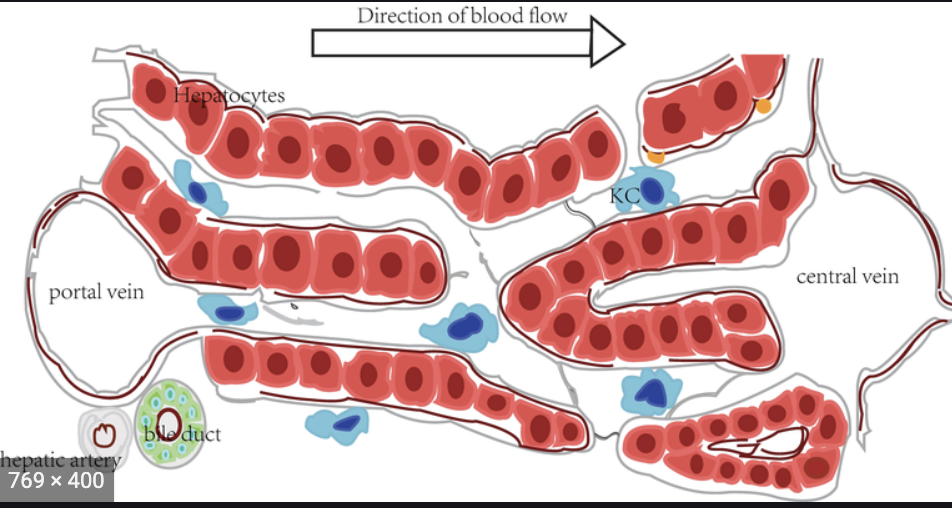
- Kupffer cells are hepatic macrophages which sit in the sinusoids b/w the portal and hepatic veins.
- Ix: Fe overload is always hypo on MR relative to the paraspinal muscles.
Diffuse liver disease: hepatic iron overload, hemosiderosis
Hepatic infection: viral hepatitis
Ix: most sens sign
- US
- CT: nonspecific findings.
- Most sens sign: hepatomegaly.
- US: hepatomeg, starry sky appearance, GB wall thickening, periportal edema.
- CT: hepatomeg, possible decreased attenuation, possible periportal/hepatoduodenal lymphadenopathy.
- MR: increased periportal T2 (edema).

DDx multiple tiny hepatic hypoattenuating lesions
- Mets
- Candidiasis
- biliary hamartomas (von Meyenberg complexes)
- Caroli disease
- lymphoma
Hepatic infection: candidiasis
Px: which organs often involved.
Ex: almost always seen in who & in particular?
Ix: CT app.
Tx: mortality?
Px: liver + spleen; invade the intestinal mucosa during periods of marked neutropenia & invade liver through the portal circulation.
Ex: immunocompromised pts., especially those w/hematologic malignancies + chemo.
Ix: CT: tiny hypoattenuating foci which may be rim-enhancing.
Tx: mortality high (30%) despite antifungals.

Hepatic infection: abscess
Px: most common general cause; common causes; less common cause; most common organism.
Ix: CT-1
MR-4
Px: bowel process; diverticulitis, appendicitis; ascending cholangitis; E. coli.
Ix: CT: ring-enhancing lesion
MR: T2 central hyperintensity, irregular wall that enhances late, perilesional enhancement.