What is shown? Name 2 possible causes.
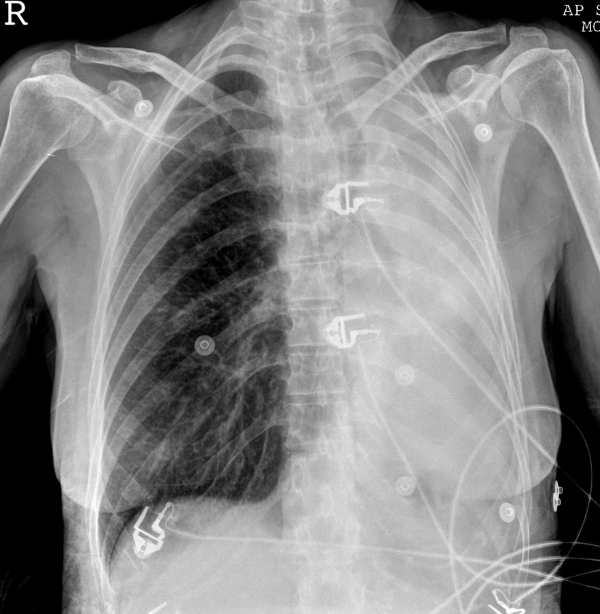
Left lung collapse/consolidation - considerable mediastinal shift to the left so there must be a considerable loss of lung volume. There is an air bronchogram of at least one of the larger bronchi indicating consolidation.
Pneumonia and obstruction of the left bronchus
What is shown on this bronchoscopy?
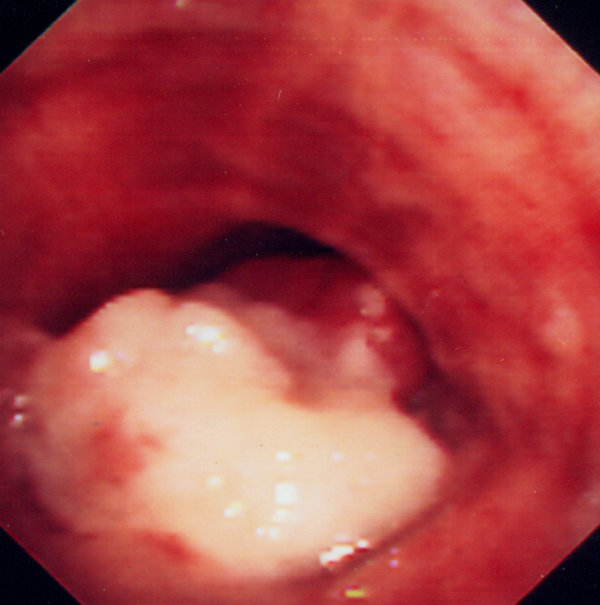
Fungating mass invading the bronchial lumen = malignant bronchial tumour
What is shown? What is the likely diagnosis? What are the main RFs?

pleural tumour encasing the lung - mesothelioma
RFs- asbestos, occupation: boilermakers, plumbers, heating engineers, electrical engineers, building work.
Where do mesotheliomas spread? (3)
Other pleural cavity
Lung
Hilar lymph nodes
Which of these is true about mesotheliomas?
- Cytology of pleural fluid at initial presentation almost always is diagnostic
- Thoracoscopy with biopsy and histology of pleura may be required
- Instillation of sclerosant substances may be used to prevent re-accumulation of pleural effusions
- Chemotherapy is highly effective
2 and 3
There are no effective treatments though instillation of sclerosants into the pleural space can prevent or reduce re-accumulation of pleural effusions and accompanying breathlessness.
What is shown?
- Lung fibrosis
- Miliary nodular lung densities
- Cavitating nodules both lungs
- Perihilar airspace oedema
- Hyperinflated lungs
- Bronchiectatic changes
What is the most likely cause?
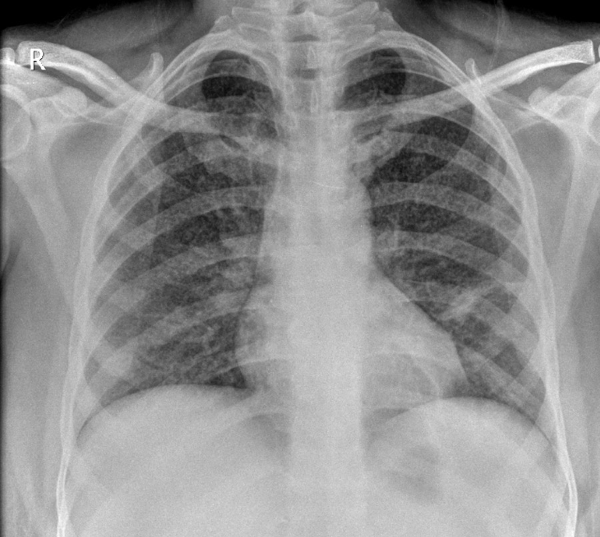
Miliary nodular lung densities - multiple nodules (1-2mm in size) throughout both lungs with patchy consolidation in left lower zone. TB is the most lilkey cause of this.
What conditions can cause miliary pattern in lung?
- TB
- Sarcoid
- Metastases
- Occupational lung disease
- EAA
What are the features of Horner’s vs 3rd nerve palsy?
Horner’s - proptosis, miosis, enophthalmos and anhydrosis
3rd nerve palsy - (superior oblique muscle) causes pupillary dilatation and a Holmes-Adie pupil (benign condition) is moderately dilated and poorly reactive to light
Horner’s syndrome with right shoulder pain which radiates to the arm is suggestive of which diagnosis?
Superior sulcus lung carcinoma/apical lung carcinoma (Pancoast tumour)
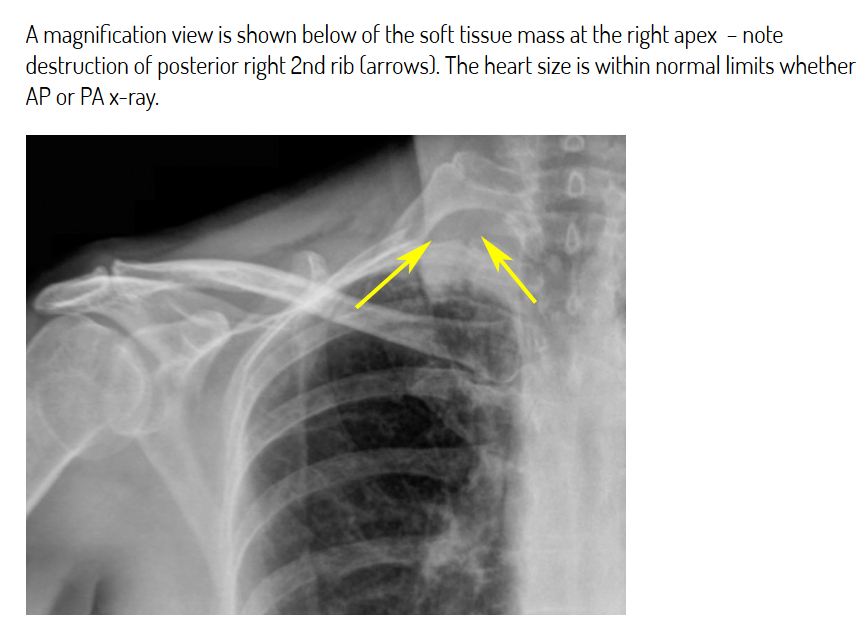
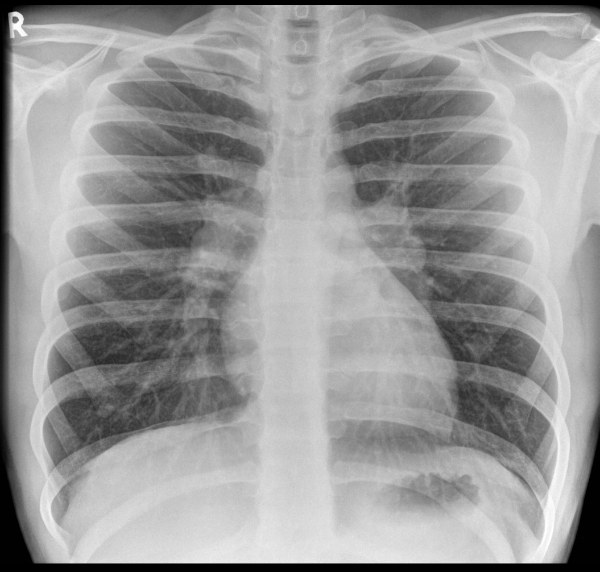
What is shown here? What is the diagnosis?
- The heart size is within normal limits
- There is abnormal soft tissue density at the right lung apex
- The left lung is clear
- Rib destruction is evident at the right lung apex
Pancoast tumour - can cause rib destruction.
Name 5 features of Pancoast syndrome.
- Invasion of the brachial plexus
- Invasion of the sympathetic chain
- Cord compression
- Invasion of the recurrent laryngeal nerve
- A hoarse voice
Pancoast tumour invading surrounding structures –> symptoms called Pancoast syndrome
Invasion starts w/ brachial plexus –> shoulder and arm pain. There may be compression of the spinal cord which occurs in 10-25% of people with Pancoast.
Which of these are associated with Horner’s?
- Diabetes mellitus
- Cerebrovascular disease
- Demyelination
- COPD
- Trauma
- Carotid aneurysm
- Carotid dissection
- Skull base tumour
All except COPD
Which 4 features are shown?
- Normal appearance
- Mediastinal shift to the left
- Large pleural effusion
- Normal heart size
- Large right-sided pneumothorax
- Large left-sided pneumothorax
- Multiple rib fractures
- Collapse left lower lobe

2, 4, 5, 8
Note collapse of left lower lobe also, probably due to mediastinal shift – this appears as a triangular area of increased density behind the hear
What can be done in large pneumothorax before insertion of chest drain? Where is it inserted?
Therapeutic aspiration of air should be undertaken (needle or venflon) to relieve tension and improve patient condition. For a pneumothorax of this size needle aspiration alone is unlikely to be sufficient and a chest-drain will be needed. This can be prepared while you aspirate air from the chest.
Sites for aspiration/drain:-
- 2nd intercostal space, mid-clavicular line
- 6th intercostal space, mid-axillary line
What is the cause of pneumothorax in COPD? Should it be drained?
Rupture of a bulla is a cause of pneumothorax especially in patients with COPD.
Yes but a large bulla can mimic a pneumothorax and should not be drained! If unsure check radiograph findings with a senior colleague.
What are the most common causes of CAP? (leading to hospital admission %)
- Strep pneumoniae (39%), followed by
- viral and C. pneumoniae (both 13%),
- mycoplasma (11%),
- H.influenzae (5%).
Other bacteria sometimes isolated are Legionella, S. aureus, Moraxella catarrhalis, C. psittici.
What are the most common types of lung cancer?
- Adenocarcinoma approx 40%
- Squamous cell carcinoma approx 25-30%
- Small cell carcinoma approx 15%
- Large cell undifferentiated approx 10%
- Rare types are bronchoalveolar carcinoma and carcinoid, both approx 1% of all tumours, and unrelated to smoking
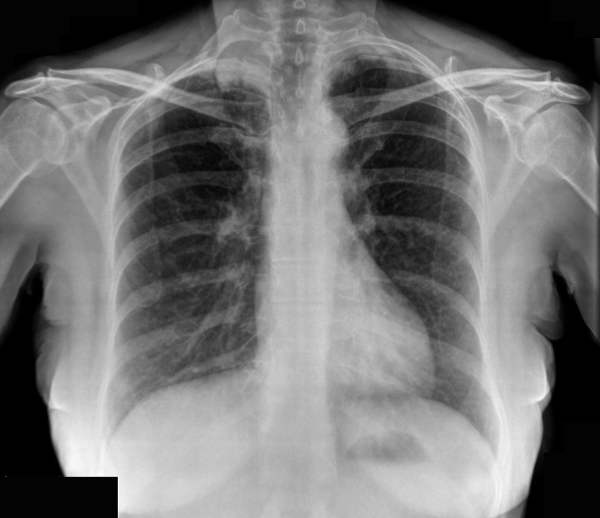
What is shown here and what are 3 causes?
This patient has prominent, bulby and symetrically enlarged hila consistent with bilateral lymphodenopathy.
Sarcoidosis/TB/lymphoma
What is shown here? Name 3 causes.

Erythema nodosum (EN).
There are rounded, erythematous and raised lesions present on the anterior shins.
EN can be associated with streptococcal infection, TB, sarcoidosis, drugs, inflammatory bowel disease and histoplasmosis.
What type of granulomatous disease is sarcoid?
Non-caseating granulomatous disease
T lymphocytes and macroophages form these granulomas. Usually causes adenopathy and parenchymal lung disease. Sometimes affects skin, eyes (uveitis and papilloedema), CNS (facial nerve palsy), heart (arrhythmias, HF, conduction).
ACE is a product of macrophages and therefore an indicator of granuloma burden in the tissues - they are correlated with disease activity.
Hypercalcaemia is present in 10% of patients and is due to increased production of 1,25-dihydroxyvitamin D by macrophages.
Which of these can cause erythema nodosum?
- TB
- Graves Disease
- Oral contraceptives
- Rheumatoid arthritis
- Cushings disease
- Crohn’s disease
1, 3, 6
-
Acute bronchitis11
-
Asthma21
-
Aspergillus lung disease30
-
ARDS11
-
Asbestos-related lung disease (incl. asbestosis and mesothelioma)24
-
Bronchiectasis18
-
COPD33
-
Extrinsic allergic alveoltis17
-
Idiopathic pulmonary fibrosis16
-
Lung Cancer43
-
Obstructive sleep apnoea19
-
Pleural Effusion16
-
Pneumoconiosis13
-
Pneumonia46
-
Pneumothorax26
-
Pulmonary Embolism22
-
Sarcoidosis15
-
MedEd - Chest pain38
-
Capsule Cases22
-
Procedures (chest drain)0
-
Smoking cessation4
-
Cavitating lung conditions2
-
X-rays6
