Describe the overall processes of the GI Tract
Metabolic processes need a specific, range of small molecules. Food has a wide range of mostly large molecules locked into complex structures. It may also be contaminated with pathogens.
Digestion makes food into a sterile (removes pathogens), neutral, and isotonic solution of small sugars, amino acids and small peptides, small particles of lipids and other small molecules. This is now ready for absorption and excretion.
Initial physical disruption –> Ingestion and rapid transport to storage –> Initial chemical disruption and creation of suspension (chyme) –> Disinfection –> Controlled release of Chyme –> Dilution and neutralisation (hypertonicity and acidity are corrected) –> Completion of chemical breakdown –> Absorption of nutrients and electrolytes –> Final absorption of water and electrolytes –> Producing faeces for controlled excretion.
Define Absorption and Excretion
Absorption: the specific active or passive uptake of nutrient molecules, water and electrolytes
Excretion: residues from food and gut debris – waste materials specifically excreted via liver to gut. They need to be processed, stored and released at an appropriate time.
Explain about Digestion
Digestion: food needs to be disrupted physically to release large molecules and broken chemically to release small molecules – so it is possible move through the digestive tract. The processes are relatively slow – we can eat much faster than we can digest so ingested food needs to be stored.
Digestion is accomplished by the action of HCl, bile and a variety of enzymes secreted by exocrine glands- secretion. While these processes are going on, the contractions of the smooth muscles in the walls of tract, mix and move the ingested food from the mouth to anus – motility.
Big Processes
- Secretion: adding to contents
- Motility: controlled movement of contents
- Absorption: removal from contents (recovering nutrients and secretions to avoid waste)
Describe the broad function of the mouth and oesophagus
Mastication: tenth can generate high pressure due to our jaws and muscles
Saliva
- Protects mouth
- Wets / Bacteriostatic / Alkaline / High Ca2+ (protects teeth)
- Lubricates food for mastication and swallowing
- Wet / Mucus
- Starts digestion
- Sugars
Swallowing
- Formation of bolus (mass of food that has been chewed at the point of swallowing)
- Rapid oesophageal transport
Describe the broad function of the stomach
Storage
- Relaxes to accommodate food
Initial disruption
- Contracts rhythmically to mix and disrupt
- Secretes acid and Proteolytic enzymes to break down tissues and disinfect
- Acid, enzymes and agitation produces chyme
- Now known as Chyme (suspension of small chemicals – part liquid and part solid mass of partially digested food and digestive secretions)
- Delivers Chyme slowly into the Duodenum
Describe the broad function of the duodenum and jejunum
Dilution and neutralisation of Chyme
- Water drawn in from ECF. Stomach impermeable, Duodenum permeable.
- Alkali (bile) added from Liver and Pancreas to neutralise acid (the common bile duct and the common pancreatic duct drain into the second part of the duodenum – major duodenal papilla)
- Pancreas, liver and intestine secrete enzymes and bile acids to complete digestion
- Completion of digestion takes place as enzymes from pancreas and intestine
- cleave peptides to amino acids
- cleave polysaccharides to monosaccharides
- Break-down and re-form lipids
- Break down nucleic aicds
Describe the broad function of the small intestine
Absorption of nutrients and electrolytes
- Fluid passes very slowly through the small intestine - may take many hours (molecules from the lumen diffuse into the layers)
- Large surface area due to brush border
- Epithelial cells absorb molecules, some actively some passive
- Often coupled to Na+ absorption
- Pass into hepatic portal circulation (First pass…) – enter the hepatic portal vein – doesn’t go back to the heart (conducted directly from the gut to the liver)
Absorbs the majority of water (12.5L vs. 1.35L large intestine)
Describe the broad function of the large intestine
Final absorption of water (1.35L)
Very slow transit
Faeces form and accumulate in the descending and sigmoid colon
Describe the broad function of rectum
Controlled excretion
Faeces propelled periodically into rectum
Urge to defecate
Controlled relaxation of sphincters and expulsion of faeces
Describe regional variation in macro and microstructure of each of the major divisions of the alimentary canal that relate to functional adaptations for transport, storage, digestion and absorption
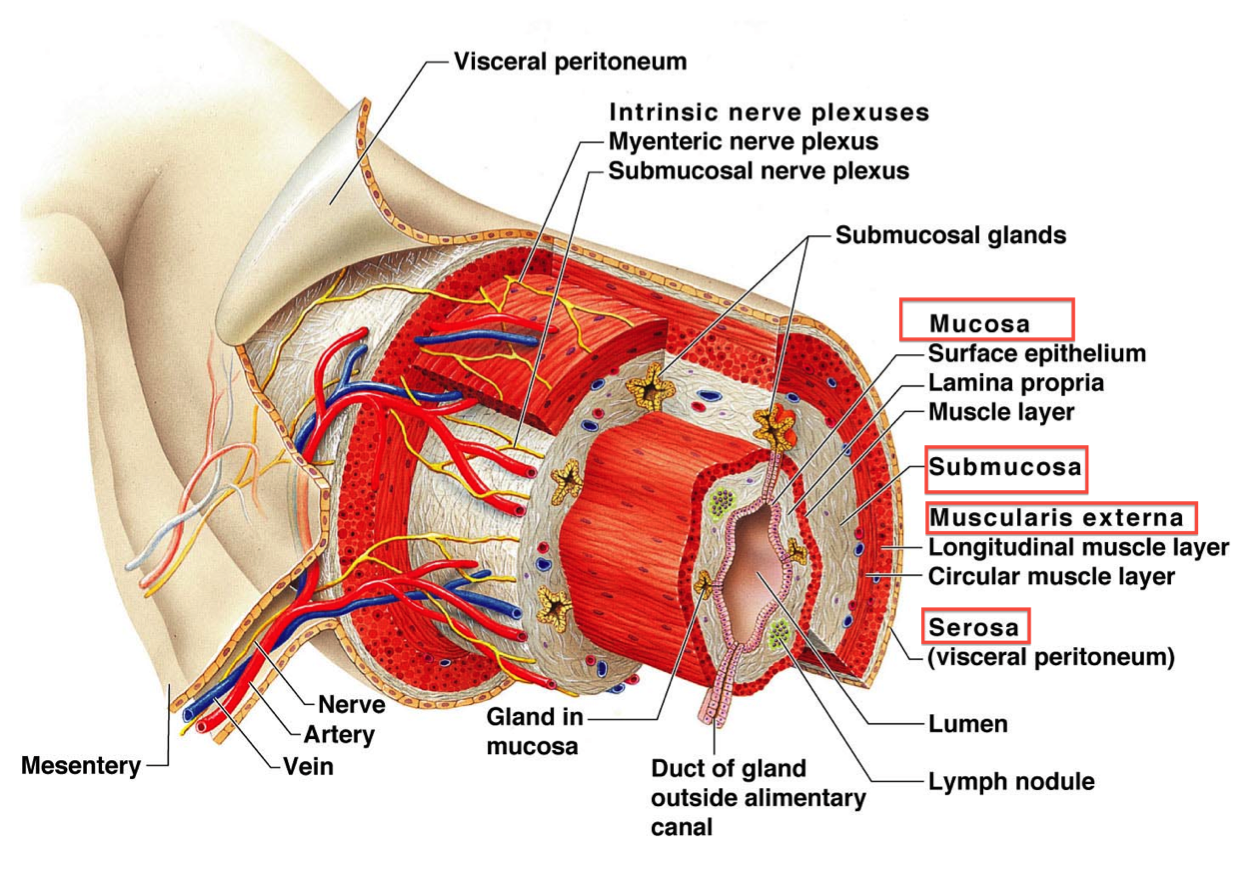
From the oral cavity (oropharynx) to the anus the alimentary canal consists of four layers (from within outwards)
- Mucosa
Epithelial lining, connective tissue and thin layer of smooth muscle
- Submucosa
Fibroelastic tissue with vessels, nerves of the submucosal plexus, lymphoycytes, leucocytes and fat cells
- Muscularis Externa
Inner circular and outer longitudinal layer of smooth muscle with the myenteric plexus lying in between the layers.
- Serosa/Adventitia
Thin outer covering of connective tissue
Variations in the cellular composition of these layers provide structural criteria to separate the alimentary canal into various regions, each with specific functions whilst continuous throughout as a hollow tube of variable diameter and shape.
Describe the Fluid Balance of the Gut
- Each day we ingest about 1kg of food and about a litre of liquids. The food is mixed with 1.5L of Saliva and about 2.5L of gastric secretions to form chyme. Chyme is very hypertonic (has a high osmotic strength) and is very acidic.
- When chyme is slowly released from the stomach, around 9L of water (and alkali) moves into it across the duodenal wall, from the ECF via osmosis.
- We eat about 1kg food per day, add about 1.5l saliva, add about 2.5l gastric secretions (including HCL and enzymes) then up to 9l of water and alkali to achieve isotonicity.
- Small intestine absorbs about 12.5L water etc, large intestine absorbs about 1.35L of water and electrolytes leaving 0.15kg faeces. (Turnover is incredibly high)
- If the balance between secretion and absorption is only slightly altered, considerable loss of water and electrolytes will occur. Mostly not from ingested food and water but from body fluids. Leading to rapid dehydration and electrolyte disturbance. In diahrrhoea you deplete your body as well fail to absorb what you have consumed
Describe the properties of the enteric nervous system and its relationship to the autonomic nervous system
The enteric nervous system is a subdivision of the autonomic nervous system that directly controls the GI system. It is made up of two nerve plexuses formed of post-ganglionic neurons in the wall of the gut, between muscles, that may act independently of the CNS (short reflex pathway). This activity may be modified by both branches of the ANS (long reflex pathway). Parasympathetic control however is the most significant. It coordinates both secretion and motility using a range of neurotransmitters, not just Ach as you may expect (parasympathetic).
Apart from the voluntary control of the muscles of chewing and of defecation the nervous control of the motility of the gut is entirely autonomic. The membrane potentials of the smooth muscle cells show continuous slow fluctuations – the basic electrical rhythm. These short waves do not initiate contraction. Contraction follows the appearance “spike potentials” initiated by reflexes mediated by the enteric nervous system.
Describe the role of hormones and other peptides which affect the motility and secretion in the gut
Endocrine cells in the walls of the gut release a dozen or more peptide hormones. These include both hormones with endocrine action and paracrine action. The hormones comprise two structurally related groups – the Gastrin group and the Secretin group. These hormones are released from one part of the gut to affect the secretions or the motility of other parts.
Paracrine: chemical messengers diffusing locally: histamine in stomach, vaso-active substances
Endocrine: range of hormones controlling secretion of acid, alkali secretion from liver and pancreas, enzyme secretion.
Explain about Dysphagia
Difficulty swallowing. May be caused by problems with the oesophagus, e.g. musculature, obstruction by tumour or neurological, e.g. a stroke. Tumours of the oesophagus, high up are Squamous Cell Carcinoma, lower down are Adenocarcinomas.
Food enters the gut by the processes of mastication and swallowing. Swallowing is a complex set of muscle contractions which form a bolus of food in the mouth then propel it towards the larynx from where it passes into the oesophagus for rapid propulsion into the stomach. The ability to swallow effectively is very important and may be compromised by anaesthesia or neurological deficits.
Liquids are more difficult to swallow, so where swallowing is compromised, liquids are often thickened to assist the process.
Explain about Acid Reflux
– Sphincter between the oesophagus and the stomach is weak, acid refluxes into the oesophagus and causes irritation and pain (heartburn).
May also cause much more serious damage to the oesophageal mucosa.
Acid leaving the stomach may also cause ulceration in the duodenum.
Explain about Barrett’s Oesophagus
Metaplasia of the lower oesophageal squamous epithelium to gastric columnar. This is to protect against acid reflux.
Explain about Oesophageal Varices
Portal venous system is overloaded due to cirrhosis, blood is diverted to the oesophagus through connecting vessels. This leads to the dilation of sub mucosal veins in the lower part of the oesophagus.
Explain about Peptic Ulceration
Area of damage to the inner mucosa of the stomach or duodenum, usually due to irritation from gastric acid.
The stomach is defended from its own acid by mucus and hydrogen carbonate secretion, but these defences may breakdown for example after infection with H Pylori, or when taking drugs which affect prostaglandin secretion or be overwhelmed by excess acid secretion.
This typically causes pain relieved by eating and ulcers may bleed or occasionally perforate.
A variety of drugs can be used to reduce acid secretion.
Explain about Pancreatitis
Inflamed pancreas, causes considerable pain. Characterised by the release of amylases into the blood stream
Explain about Jaundice
Liver cannot excrete bilirubin, which accumulates in the blood. If build up of bilirubin is due to excess haemoglobin breakdown it is Pre-hepatic Jaundice.
If build up of bilirubin is due to bile duct obstruction and back up of bile causing liver damage it is Post-hepatic or Obstructive Jaundice.
The liver may also be damaged by disease (infection or damage by alcohol or other drugs) causing hepatic jaundice.
The secretions of the liver form bile which has both digestive and excretory functions and enter the duodenum via the major duodenal papilla. Bile acids mainly assist with digestion of fats in the intestines and are then re-absorbed in the terminal ileum and recycled to the liver, where they are immediately re-secreted in bile.
This bile is then stored until the next meal in the gall-bladder before being released to begin the cycle again. The liver also excretes bilirubin, a breakdown product of Hb.
Alcohol in particular may cause serious liver damage, leading to fibrotic changes known as cirrhosis. This leads to loss of liver functions but may also impair the flow of blood from the hepatic portal vein through the liver to the systemic venous circulation, causing portal hypertension. This may lead to the formation of ascites and also increased flow through collateral venous pathways around the oesophagus and anus.
Explain about Gallstones and Pancreatic Tumours
Precipitation of bile acids and cholesterol in the bladder forms gall stones. Often asymptomatic, but may move within the gall bladder causing painful Biliary Colic, or move to obstruct biliary outflow. Tumours of the pancreas may also obstruct biliary outflow.
- The prognosis for patients with pancreatic tumours is especially poor. The pancreas secretes alkali and a cocktail of enzymes including amylases which break down carbohydrates.
Explain about Malabsorption
Several conditions affect how well the intestines can absorb things.
The remainder of the small intestine (after the major duodenal papilla) is the principal site of absorption. Neutral chyme is propelled gently along its length by segmentation and the large surface area allows a complex of absorptive processes to occur.
The motility of the ileum may be compromised under some circumstances, leading to paralytic ileus and it may also become obstructed either from an internal obstruction or external compression.
Explain about Appendicitis
Inflammation of the appendix, presents as a sharp pain in the side at the same level as T10, which then localises to the right lower quadrant (where the appendix is located)
Explain about Peritonitis
Inflammation of the peritoneum.
- The major parts of the gut are enclosed in a virtual space created by the peritoneum.
- Peritonitis will normally follow any perforation of the gut as the contents are released into the space.
