Steps of the Whipple – Excisional phase
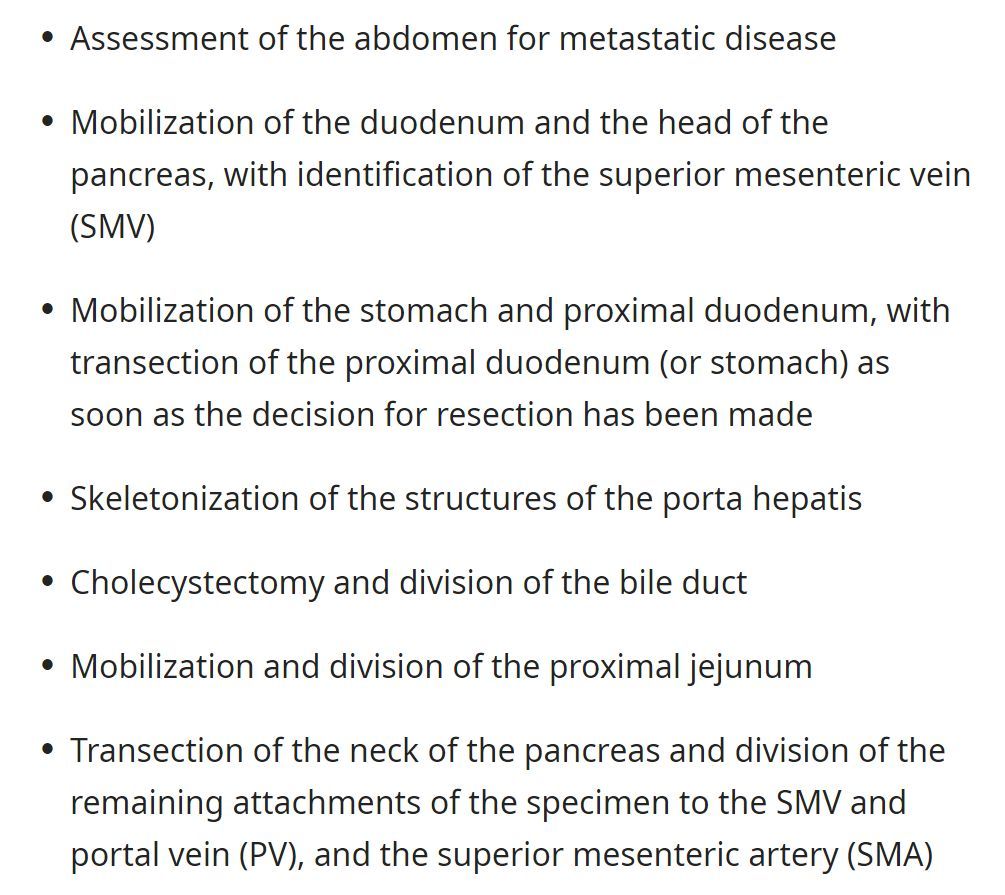
“Classic” vs “Pylorus-preserving” Whipple procedures
“Classic” removes the pylorus and the antrum of the stomach, leaving the proximal stomach.
“Pylorus preserving” removes the duodenum up to a small pre-pyloric region, preserving the entirety of the stomach.
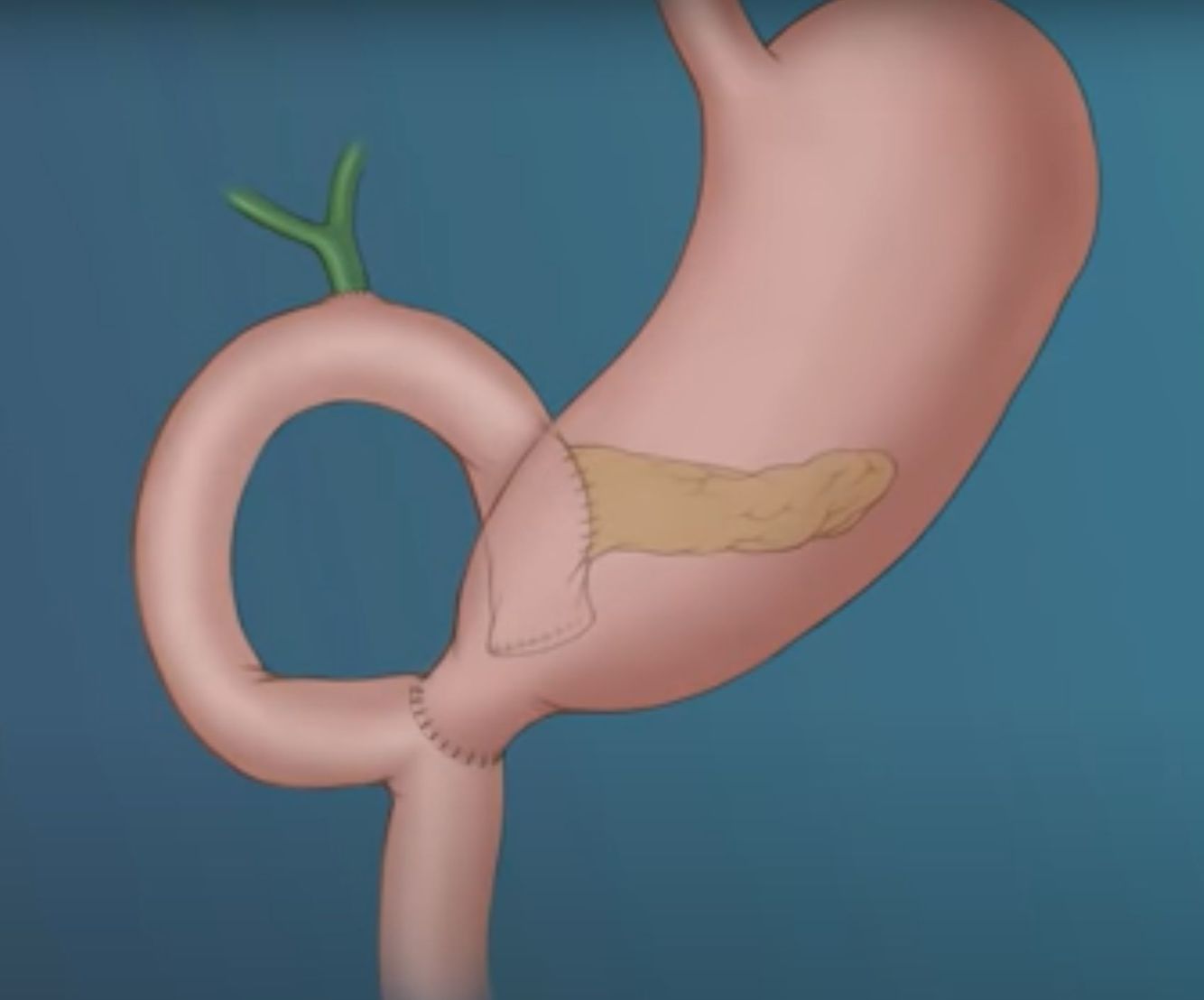
Steps of the Whipple – Reconstruction phase
- Reconnect the remaining pancreas to the jejunum in an end-to-side anastamosis
- Reconnect the common hepatic duct to the jejunum in an end-to-side anastamosis
- Reconnect the pylorus (or stomach) to the jejunum downstream of the bile duct anastamosis
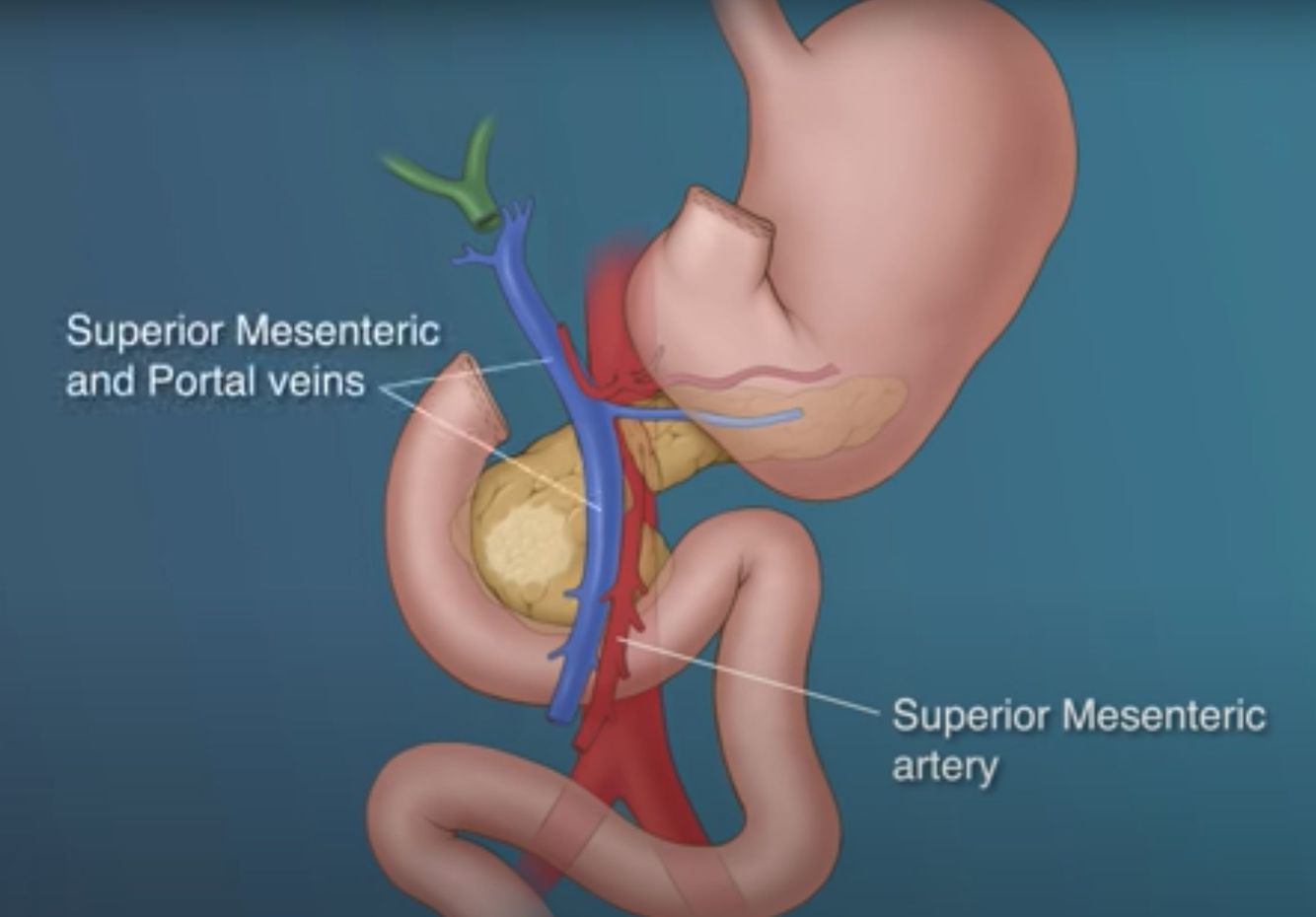
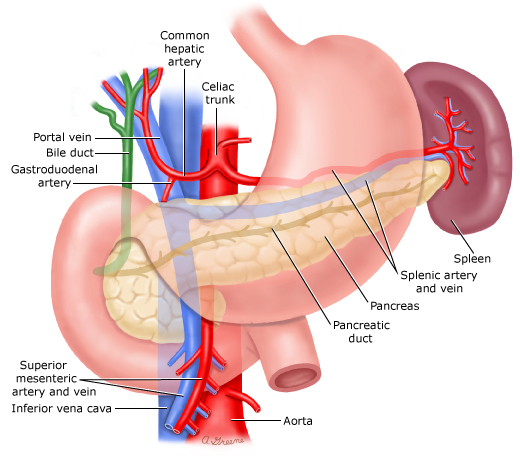
Vessels at risk of invasion in pancreatic head malignancy
- Superior mesenteric artery
- Superior mesenteric vein
- Portal vein
Islet density is highest in the __ of the pancreas
Islet density is highest in the tail of the pancreas
Pre-operative biliary decompression in obstructive jaundice
- Mixed evidence in the medical literature.
- Most surgeons reserve this for:
- When bilirubin exceeds 20 mg/dL
- When surgery must be delayed for two weeks or more
- When there is debilitating pruritis or cholangitis
Indications for Whipple
- Pancreatic adenocarcinoma
- Cholangiocarcinoma
- Ampullary carcinoma
- Obstructive Ampullary adenoma
- Duodenal malignancy
- Rarely for large neuroendocrine tumors of the pancreas
- Combined pancreatic-duodenal injury in trauma
- Chronic pancreatitis (Chronic pain, non-dilated duct, failed endoscopic therapy)
Pre-operative biliary stenting for patients with obstructive jaundice scheduled to undergo Whipple
- Plastic stents are preferable, as metal stents tend to induce an inflammatory response and become incorporated into the bile duct wall (making them hard to remove intraoperatively)
- Care should be taken not to place the stent too high in the common bile duct, as this may complicate the surgery.
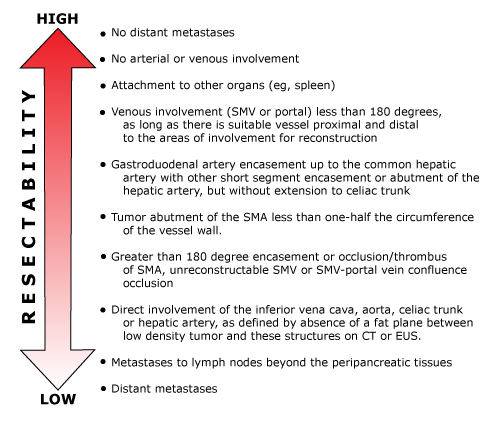
Resectability of pancreatic adenocarcinoma
Anatomy of pancreatic adenocarcinoma
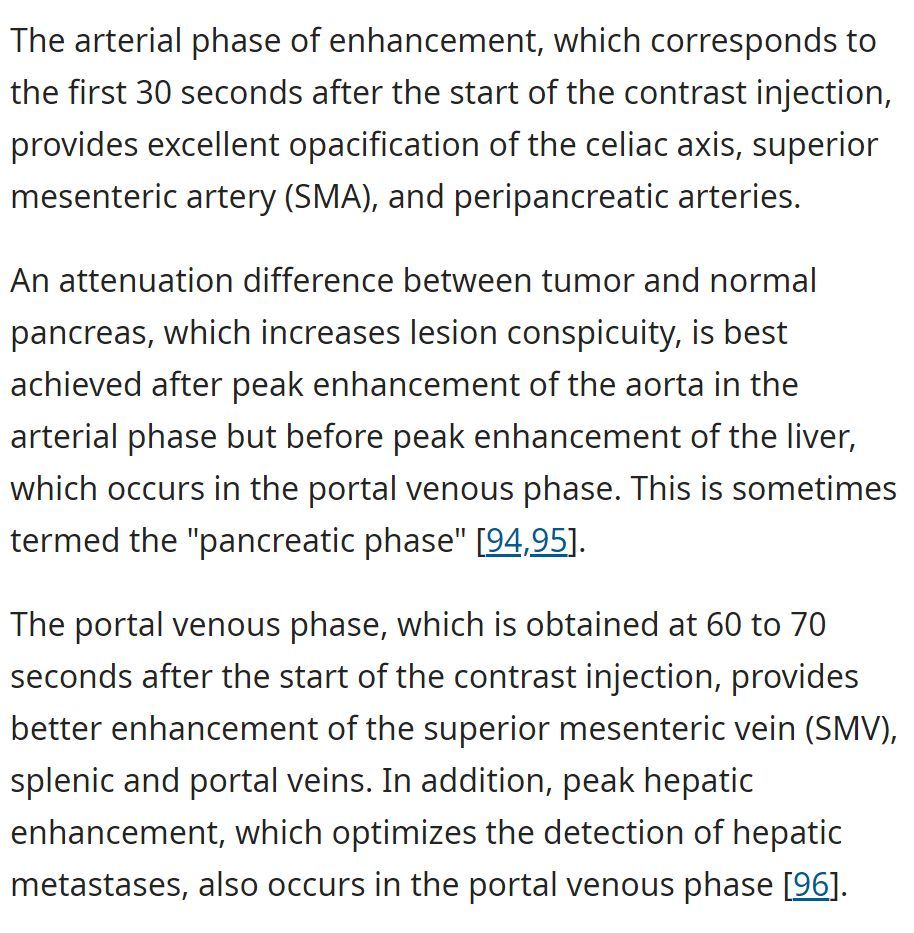
Preferred method to stage pancreatic cancer
Three-phase CT
Main vascular contraindications to Whipple
- Envasement of a vessel (SMV, portal vein, > 180 degrees SMA)
- Occlusion or thrombosis of the SMV
- SMV-portal vein confluence
Role of biopsies in pancreatic malignancy
- A diagnostic biopsy of a suspected pancreatic malignancy may be indicated if:
- There is evidence of systemic spread of disease
- There is local evidence of unresectability on staging studies
- The patient is unfit for major surgery
- Neoadjuvant treatment is being contemplated
- However, a preoperative diagnostic biopsy may not be needed in a fit patient with a potentially resectable pancreatic lesion that is highly suspected of malignancy
- Biopsies are highly specific, but not entirely sensitive
Preparation for the Whipple
- NPO from midnight
- Prophylactic antibiotics (probably cefazolin + metronidazole)
- Subcutaneous lovenox and pneumoboots for thromboprophylaxis
Some surgeons begin the Whipple procedure as. . .
. . . staging laparoscopy
To ensure that the disease is resectable – as imaging may miss liver or peritoneal metastasis.
However, these laparoscopies are poorly sensitive for vascular invasion, which can also be a contraindication to resection.
If you go in for a Whipple, but disease is found to be unresectable, what should you do?
Typically the opportunity will be taken to preform an appropriate palliative surgery instead – such as gastrojejunostomy or biliary bypass
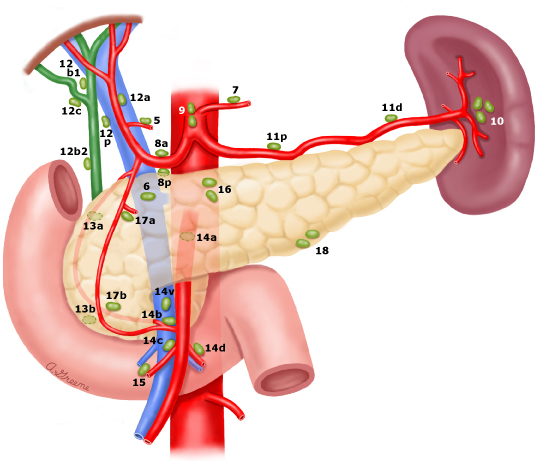
Lymph nodes in pancreatic head malignancy
The standard regional lymph node basin for tumors located in the head and neck of the pancreas includes those along the common bile duct; common hepatic artery; portal vein; pyloric, posterior, and anterior pancreaticoduodenal arcades; and along the superior mesenteric vein and right lateral wall of the superior mesenteric artery
Evaluation of a minimum of 12 lymph nodes is recommended to accurately stage N0 tumors. (1-3 positive nodes is N1, >4 is N2)
Nodes outside of this area are considered distant metastases. If one is found to be positive, the operation is aborted.
Rationale of placing a drain after Whipple
To provide controlled external drainage of a pancreatic leak.
Inadequate drainage of a leak can lead to an intra-abdominal abscess.
Enucleation of small pancreatic head lesions
- < 1 cm benign pancreatic head lesions may be enucleated to avoid unnecessary pancreaticoduodenectomies
- This should not be performed for any lesion greater than 2 cm or any lesion suspicious for malignancy
- Most commonly performed for neuroendocrine tumors, like insulinomas and gastrinomas
- Generally well tolerated, but suprisingly the rate of pancreatic fistulas is higher after enucleation than after Whipple
Postoperative management following a Whipple
- Most stay 7-10 days
- Oral feeding is preferred, if possible (if not, jejunostomy), starting with a clear liquid diet on POD 1 or 2, then normal diet on POD 3-5
- Drain management (see separate card)
- Most patients will not need enzyme supplementation, but if steatorrhea develops then Creon and PPI may be perscribed
- Conflicting data over whether or not somatostatin analogues reduce the post-operative rate of pancreatic fistula formation
Drain management following Whipple
- Should be straw-colored or clear
- If green, there is a bile leak
- If cloudy/turbulent, pancreatic leak should be suspected.
- On this fluid, obtain an amylase
- Fluid amylase > 3x the ULN serum amylase on or after POD#3 defines a pancreatic leak
- High amylase also suggests high probability of later fistula formation
- If no evidence of bile or pancreatic leak, drain can be removed once the patient is tolerating a normal oral diet
Most post-operative biliary and pancreatic fistulas. . .
. . . close spontaneously in 4-6 weeks
If there is a leak but the patient is otherwise ready for discharge, they may be discharged with the drain in place and can be removed at a later date once the fistula has resolved.
Patient is POD#3 following a Whipple. The procedure was uncomplicated and they are generally recovering well. However, they have persistent vomiting when taking food PO. Patient history includes prior cholecystectomy and type II diabetes mellitus. What are the next steps? What is the likely diagnosis?
- Likely diagnosis: Delayed gastric emptying following Whipple. Occurs in ~25% of patients following this procedure.
- Next steps:
- CT to rule out gastric obstruction due to fluid collection
- Conservative therapy
- Exact etiology is unclear. Fluid collections or pancreatic anastamosis may mimic this condition, and alkaline reflux gastritis may contribute to the pathophysiology.
Rates of relevant post-operative complications in Whipple patients
- Pancreatic leak/fistula: 5-10%
- Bile leak: 1-3%
- Delayed gastric emptying: ~25%
- New onset diabetes (Type 3c): ~16%
- Pancreaticojejunal anastamotic stricture: 1 - 11%
- Abscess: ~1%
- GI hemorrhage: ~3%

-
Procedural Anatomy6
-
Vascular Supply and Lymphatic Drainage15
-
Peri-Operative Risk Assessment49
-
Hematopathology62
-
GYN Onc46
-
Perioperative Antiplatelet and Anticoagulant Management42
-
Anesthetic Pharmacology60
-
Myelodysplastic syndrome5
-
Transfusion Medicine5
-
Pre-procedural and diagnostic imaging12
-
Postoperative Issues88
-
Liver, Gallbladder, Pancreas103
-
Trauma and Wound Management140
-
Drug Reactions3
-
Electrolytes6
-
Intensive Care62
-
Esophagus, Stomach, Pharynx, Oral Cavity68
-
Abdominal Pain117
-
Nonconventional Dysplasia in IBD10
-
Chronic GI and GI Bleeds122
-
Vascular Disease and Vascular Surgery70
-
Drugs for Cancer and MDS3
-
Bites and Stings9
-
Toxic ingestion10
-
Surgical Management of Endocrinopathies94
-
Neurosurgery27
-
Useless things that they want us to know9
-
Burns, Hypothermia, Frostbite28
-
Orthopedics82
-
Hernias32
-
Head and Neck Surgery41
-
Anesthesia Curriculum71
-
Bladder, Kidney, Ureter, Urethra32
-
Ophthalmology13
-
Bariatric Surgery13
-
Lung Surgery60
-
Pediatric Surgery30
-
Urology77
-
Whipple33
-
Treating valve disease9
-
Emma Holiday Review66
-
Uworld Last Week5
