AJCC
T4a group for breast carcinomas includes carcinomas with __. This does not include ___.
Invasive carcinomas greater than __ mm and less than or equal to __ mm are staged as T2; those greater than __ mm are T3.
The AJCC T4a group for breast carcinomas includes carcinomas with extension to the chest wall. This does not include invasive carcinomas adhering to or invading the pectoralis muscle. The carcinoma must penetrate beyond the pectoralis muscle into the chest wall to be classified as T4a. Invasive carcinomas greater than 20 mm and less than or equal to 50 mm are staged as T2; those greater than 50 mm are T3.
Is it positive for CK 5/6?
What is the risk of a radiologically occult invasive carcinoma?
Is sentinel lymph node procedure is not recommended?
It exhibits ___ nuclear grade.
Is comedo necrosis is common?.
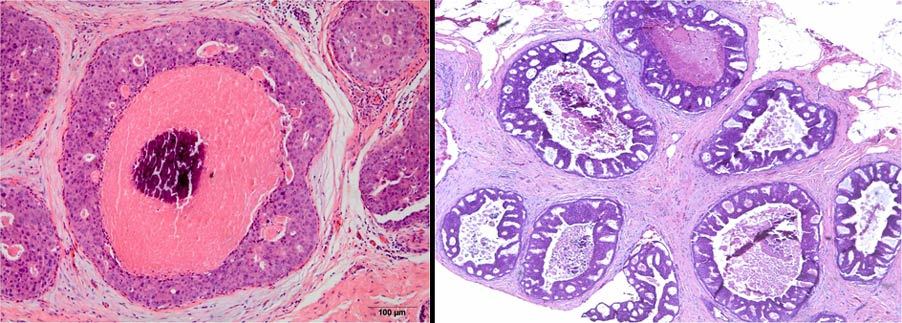
High grade DCIS is non-reactive with CK 5/6 as opposed to ductal hyperplasia which shows significant positivity.
The risk of occult invasive carcinoma in high grade DCIS is about 50%, and, therefore, sentinel lymph node procedure is recommended in those cases.
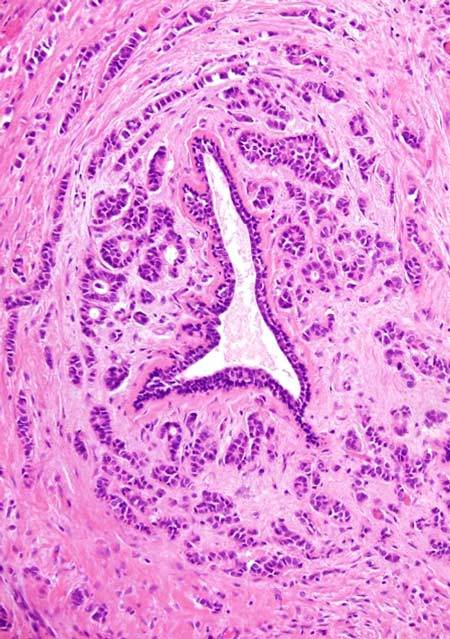
Which immunohistochemical markers are most useful in distinguishing between benign and atypical epithelial foci within papillary proliferations of the breast?
ER and CK5 staining, when used together, are valuable adjunct stains to differentiate usual duct hyperplasia from atypical proliferations within papillary lesions on breast core biopsy.
- Diffuse ER expression with lack of CK5 staining is seen in atypical epithelial proliferations.
- Mosaic expression of both ER and CK5 is generally encountered in usual hyperplasia.
Hormone receptor assay and reporting
- The CAP recommends that the cold ischemia time of ___ or less.
- Samples should be fixed for at least __ to a maximum of __ hours for receptor stability.
- Positivity for ER or PR is based on finding of __% immunoreactive tumor cell nuclei.
- A specimen may have to be rejected if __
- The CAP recommends that the cold ischemia time be kept to one hour or less.
- Samples should be fixed for at least 6 hours to a maximum of 72 hours for receptor stability.
- Positivity for ER or PR is based on finding of ≥1% immunoreactive tumor cell nuclei.
- A specimen may have to be rejected if the slide lacks staining of included normal epithelial elements and/or normal positive control on same slide.
According to the 2007 ASCO/CAP guidelines for Her2/neu testing, a Her2/neu positive result includes at least one of the following:
- Immunohistochemical staining of __+ (uniform, intense membrane staining of >__% of invasive tumor cells
- FISH result of more than __ HER2 gene copies per nucleus
- FISH ratio (HER2 gene signals to chromosome 17 signals) of more than __
According to the 2007 ASCO/CAP guidelines for Her2/neu testing, a Her2/neu positive result includes at least one of the following:
- Immunohistochemical staining of 3+ (uniform, intense membrane staining of >30% of invasive tumor cells
- FISH result of more than 6.0 HER2 gene copies per nucleus
- FISH ratio (HER2 gene signals to chromosome 17 signals) of more than 2.2.
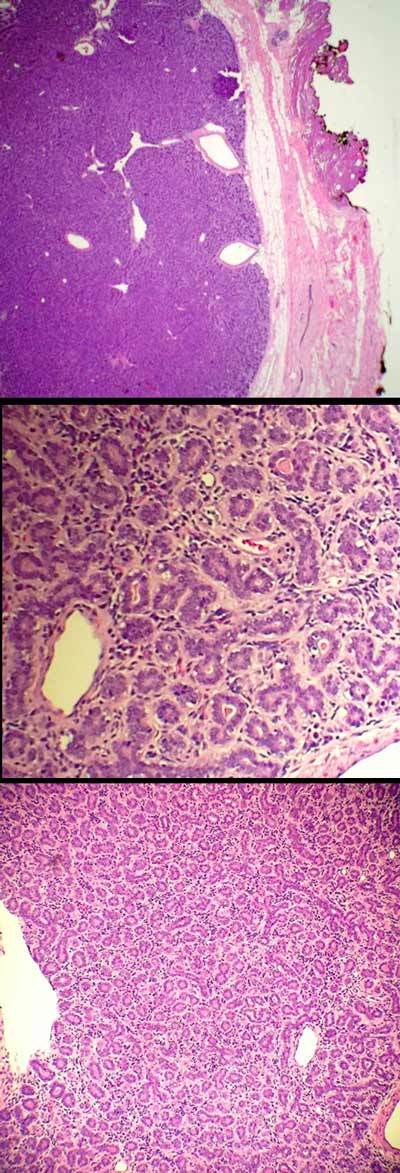
Adenoid cystic carcinoma (ACC) of the breast
- Incidence?
- Age?
- Hormone receptor profile?
- Clinical course?
- More aggressive behavior can be seen in the __ variant
- Morphologically, ACCs of the breast are similar to those seen in salivary glands, composed of two cell types
- one which stains with luminal epithelial markers ____ (4)
- the other staining with ___ (4) and ___(4)
- ACCs of the salivary gland and breast consistently harbor the hallmark __ fusion gene resulting from a __ translocation.
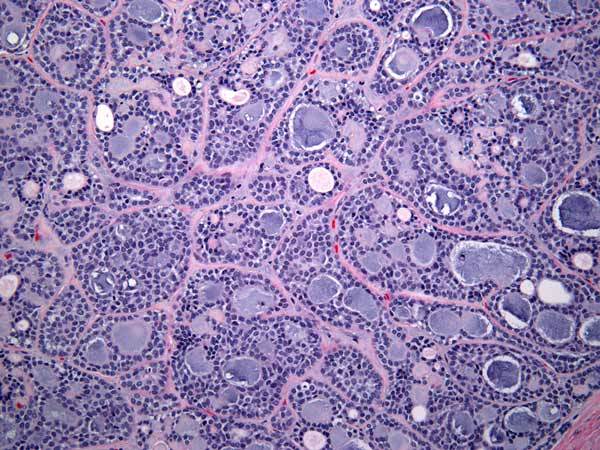
Adenoid cystic carcinoma (ACC) of the breast
- rare tumor accounting for less than 0.1% of all breast carcinomas
- occurs predominantly in postmenopausal women (mean age of 60)
- triple negative (ER/PR/HER2) receptor profile
- indolent clinical course, presenting with localized disease
- more aggressive behavior can be seen in the solid variant
- Morphologically, ACCs of the breast are similar to those seen in salivary glands, composed of two cell types
- one which stains with luminal epithelial markers CK7, EMA, CEA, and CD117
- the other staining with high molecular weight/basal cytokeratins CK5, CK5/6, CK14, CK17 and myoepithelial markers p63, S100, actin, calponin
- ACCs of the salivary gland and breast consistently harbor the hallmark MYB–NFIB fusion gene resulting from a t(6;9)(q22–23;p23–24) translocation.
Small cell carcinoma breast primary v. met
Similar?
Distinguising?
Small cell carcinoma breast primary v. met
Similar
- expression of pan-cytokeratin in a dot-like paranuclear staining pattern
- immunoreactive for CAM5.2, CK7, synaptophysin and TTF-1
- negative for CK20
- +/- ER/PR positivity
Distinguising?
- presence of DCIS with similar cytologic features
Dx?
E-cadherin staining?
Tubulolobular carcinoma.
- shows abortive tubule formation in addition to the characteristic single file pattern
- demonstrates intense membranous staining for E-cadherin in both the tubular and lobular components, similar to that seen in infiltrating ductal carcinoma.
- DDx
- Histology
- Staining
- Genetics
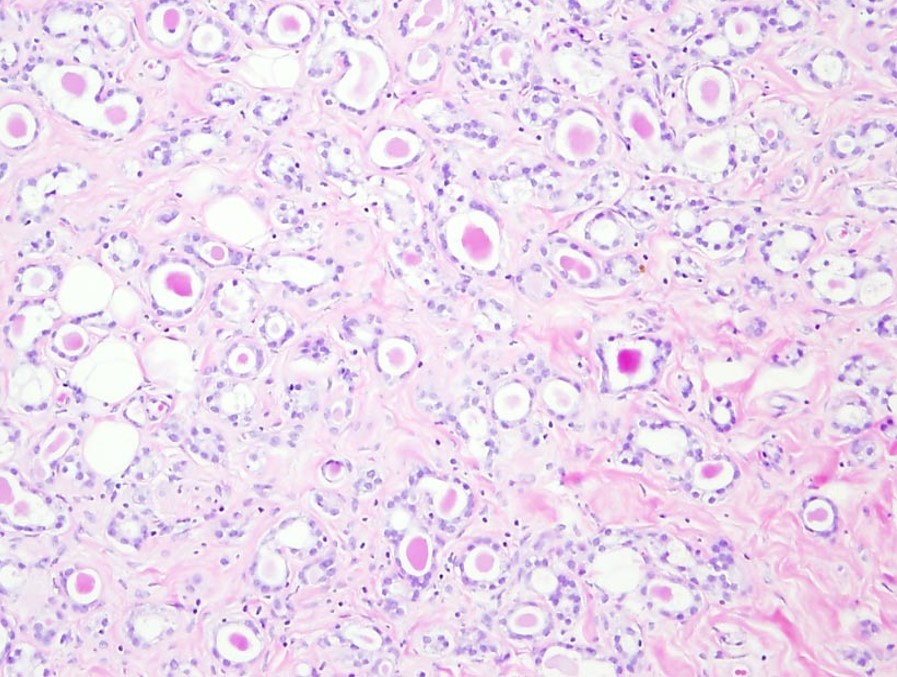
Microglandular adenosis
- DDx: invasive tubular carcinoma
- proliferation of small round glands composed of a single layer of epithelial cells surrounded by a basement membrane
- glands lack both myoepithelial cells and a lobular architecture
- not associated with a desmoplastic stroma
- strong S100 expression and a triple negative (ER/PR/HER2) receptor profile
- Chromosomal aberrations suggest the lesion to be a neoplastic clonal lesion and a possible precursor of a subset of breast cancers
DDx?
Histology?
Tubular adenoma
- circumscribed proliferation of closely packed tubules lined by two cell layers, epithelial and myoepithelial
- benign neoplasm related to fibroadenoma
DDx
Tubular carcinoma
- haphazard infiltration of bland tubules with angular contours
- Individual cells often show apical snouts
Microglandular adenosis
- comprised of infiltrating, uniform, round tubules which contain central eosinophilic secretion and which do not exhibit a myoepithelial layer.
Adenomyoepithelioma
- circumscribed proliferation of both myoepithelial and epithelial cells, the proportions of which vary
- myoepithelial cells may be either closely associated with epithelial tubules, or they may be present as aggregates of spindle, polygonal, or clear cells
DDx?
Age?
Genetics?
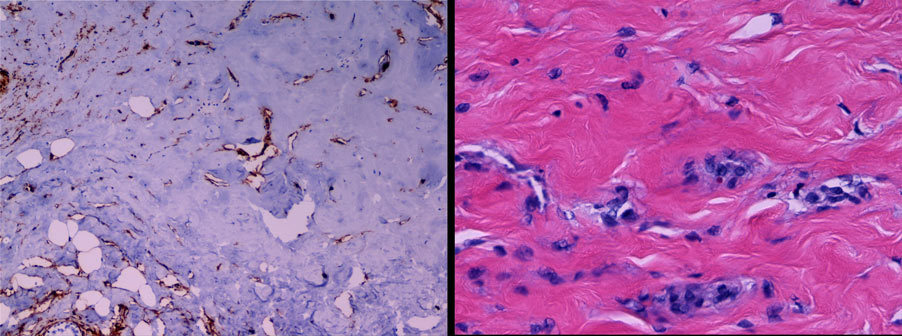
Primary (de novo) angiosarcoma of the breast
- rare, occurring almost exclusively in women with a median age of 40
- occur in the breast parenchyma, often presenting as a painless mass
- no myc amplification
- histologic grading does not correlate with clinical behavior and outcome
Secondary (radiation-associated) angiosarcoma
- occurs predominantly in the skin following surgery and radiotherapy
- median latent stage is 5-6 years
- myc amplification
- must be differentiated from atypical post-radiation vascular proliferation (APRVP)
APRVP
- generally follows a benign clinical course
- no myc amplification
Stains?
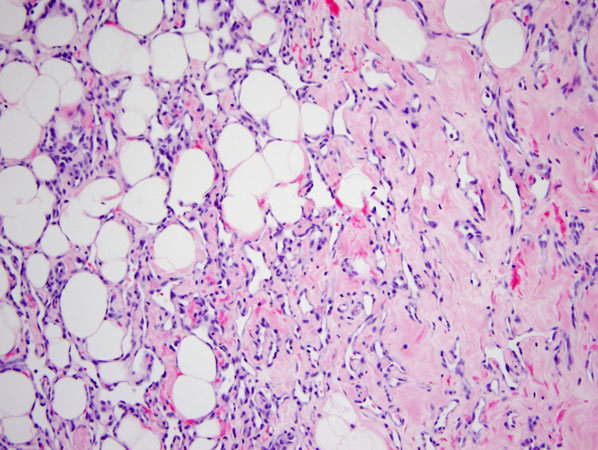
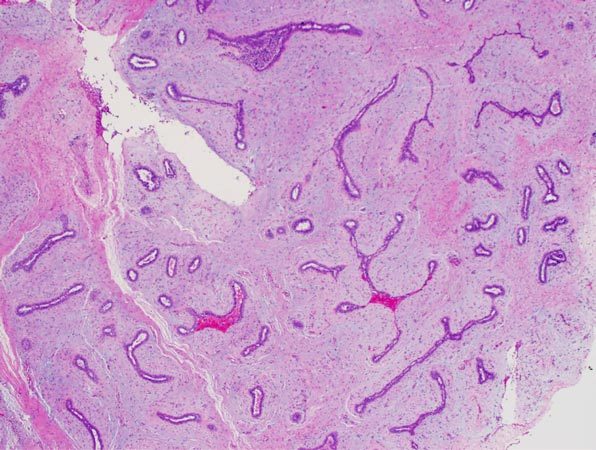
Pseudoangiomatous hyperplasia (PASH)
- benign mesenchymal proliferation
- frequently an incidental histologic finding
- rarely, it can present as a mass
- slit-like spaces
- positive for CD34, SMA, BCL-2
- negative for CD31
- not associated with microcalcifications
DDx?
Best IHC panel?
Best single stain?
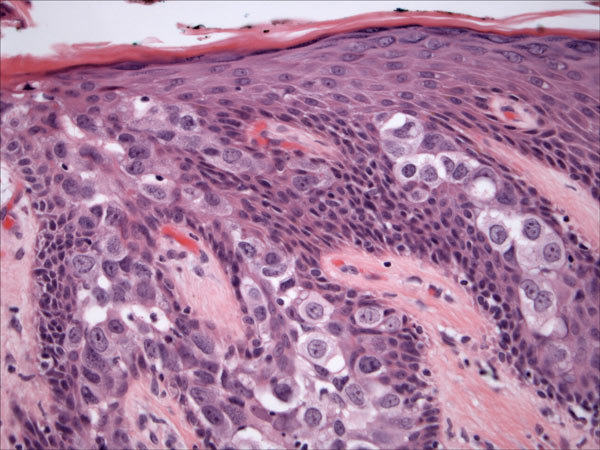
Paget’s disease of the nipple
- the presence of carcinoma cells in the keratinizing epithelium of the nipple, often with ductal carcinoma in situ involving the adjacent lactiferous ducts
- Invasive or in situ carcinoma is present elsewhere in the breast in >90% of cases
DDx
Paget’s
- Positive: HER2, CK7, CAM5.2, CEA, +/-S100
- Negative: ER, HMB45, Melan-A, CK5/6, CK20
Toker cells
- Positive: ER, CK7, CAM5.2, CEA, +/-S100
- Negative: HER2
Squamous cell carcinoma in situ/Bowen’s disease
- Positive: CK5/6, CK20
- Negative: HER2
Melanoma
- Positive: HMB-45, Melan-A
- Negative: HER2
Best 4 stains (all negative in Paget’s)
- HMB-45, Melan-A, CK5/6, CK20
HER2 is the most useful single immunostain
- positive in up to 80-90% of Paget’s disease
- negative in the other entities in the differential
What is the typical immunoprofile of in situ and invasive lobular carcinoma? (E-cadherin, catenin P120)
Lobular neoplasia, including both in situ and invasive lesions
- typically lacks membranous staining for both E-cadherin and catenin P120
- typically display positive cytoplasmic staining for P120
Dx?
Incidence?
Prognosis?
Pure or mixed?
ER, PR and Her-2?
Age?
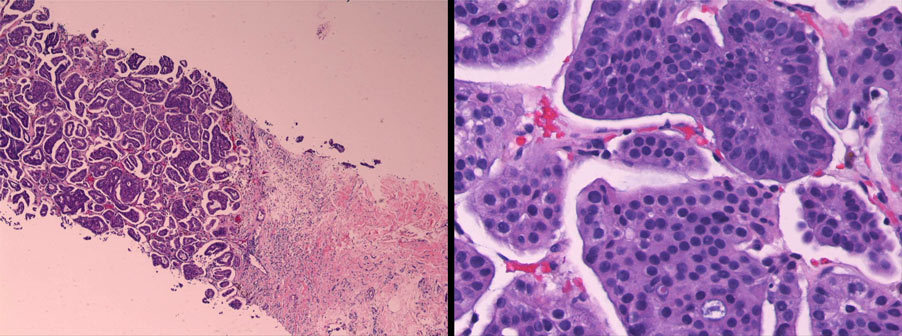
Invasive micropapillary carcinoma
- relatively uncommon
- highly aggressive
- mostly occurs in mixed form with other types of invasive ductal carcinoma
- >50% of cases are ER, PR and Her-2 positive
- no specific age range
According to AJCC staging guidelines:
Metastases in 1 to 3 lymph nodes with at least one greater than 2.0 mm should be staged as ___
Isolated tumor cells (ITCs)
- =__ cells, = __ mm
- __ when alone
- if other lymph nodes contain micro- or macrometastases, nodes with ITCs __ included in the total lymph node count for determining pN stage
Micrometastases
- tumor foci > __ cells or __ to __ mm
- pNmi when alone
- with at least one other metastasis > 2.0 mm, they __ included in the total lymph node count for the pN stage
Isolated tumor cells (ITCs)
- =200 cells, = 0.2 mm
- pN0(i+) when alone
- if other lymph nodes contain micro- or macrometastases, nodes with ITCs are NOT included in the total lymph node count for determining pN stage
Micrometastases
- tumor foci > 200 cells or 0.2 to 2.0 mm
- pNmi when alone
- with at least one other metastasis > 2.0 mm, they ARE included in the total lymph node count for the pN stage
Metastases in 1 to 3 lymph nodes with at least one greater than 2.0 mm should be staged as pN1a
Dx?
Stains?
DDx?
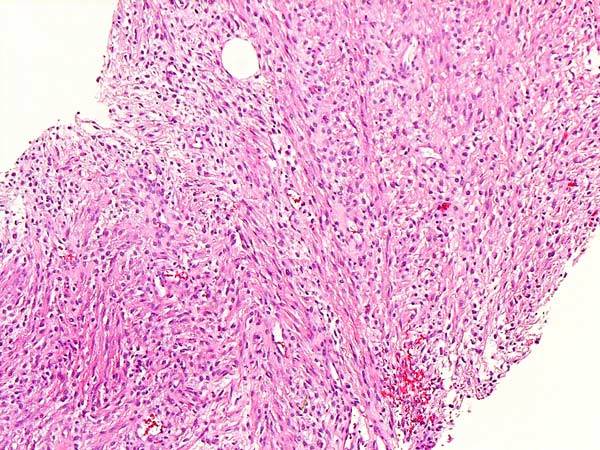
Spindle cell carcinoma
- type of metaplastic carcinoma of the breast
- positive: high molecular weight keratins (CK5/6) and the myoepithelial cell marker p63
- may be positive for only one of these markers and also show only focal positivity
DDx
- Malignant spindle cell neoplasm
- Sarcoma
- Malignant phyllodes tumor
- Nodular fasciitis
Despite that it is rare to be associated with an atypical proliferative lesion, when it occurs, the most common atypical lesion encountered is __
Although atypical or neoplastic proliferations are not often encountered in fibroadenomas, when they occur, lobular carcinoma in situ (LCIS) is most common.
Dx?
How is it detected?
Prognosis?
Treatment?
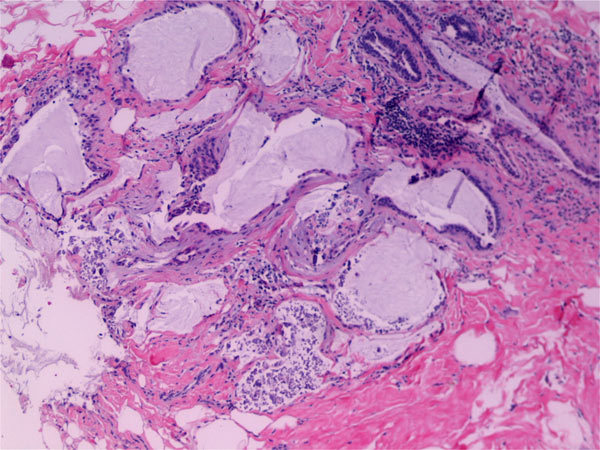
Mucocele-like lesion
- mucinous lesion of the breast with highly variable upgrade rates to atypia and malignancy on excision
- clinically occult and presents with microcalcifications on imaging
- not considered a premalignant lesion
- often associated with ADH and, therefore, follow-up excision is commonly recommended
Basal phenotype breast cancer
- characterized by __
- ER, PR, HER2?
- age
- race
- mets
- prognosis
Basal phenotype breast cancer
- characterized by the expression of one or more high molecular weight, or “basal”, cytokeratins such as CK5/6, CK14, and CK17
- most are triple negative; however, not all basal cancers are triple negative, and not all triple negative cancers are basal phenotype
- tend to affect younger patients
- more common in African-Americans
- greater propensity for brain and lung metastasis
- most have a worse prognosis
- adenoid cystic and secretory carcinoma have a favorable prognosis
Luminal A/B tumors
Luminal A tumors
- high expression of estrogen receptor and progesterone receptor positivity
- low proliferation, primarily low grade
- good prognosis
- show low benefit from chemotherapy (pathologic complete response of 0% to 5%)
Luminal B tumors
- lower level of estrogen receptor expression
- high proliferation
- possible HER2 positivity
- intermediate to poor prognosis
- intermediate benefit from chemotherapy (pathologic complete response of 10% to 20%).
Basallike breast cancers
Basallike breast cancers
- typically triple-negative
- by IHC 10% may be ER/PR+
- highly proliferating, high-grade tumors
- 80% of BRCA1 germline–associated tumors with poor outcome but with associated benefit from chemotherapy (pathologic complete response of 40%).
HER2-positive tumors by gene expression profiling
HER2-positive tumors by gene expression profiling
- 70% to 80% HER2+ by IHC and FISH
- high proliferation, high grade, and poor outcome
- benefit from chemotherapy (pathologic complete response of 25% to 40%) but not as much as basal tumors
- may express estrogen receptor–related or progesterone receptor–related genes
Molecular apocrine–type breast cancers
Molecular apocrine–type breast cancers
- some histologic apocrine features
- gross cystic disease fluid protein (GCDFP-15) positive
- estrogen receptor negative
- androgen receptor positive
- high proliferation and grade
- poor prognosis








-
Microbiology121
-
Mycology55
-
GU107
-
Lefkowitch163
-
Genetics and Syndromes49
-
Mycobacteria51
-
Parasite4
-
Pulmonary4
-
Autopsy14
-
Gyn37
-
Blood Bank17
-
Breast38
-
Cytopath61
-
Derm137
-
Bone and Soft tissue107
-
Koneman103
-
Neuro52
-
Staging36
-
Head and Neck82
-
Ro3
-
Stains58
-
GI36
-
EM9
-
Stats and Lab Management7
-
Chemistry86
-
Heme/Coag44
-
Bone and Soft tissue COPY107
-
Bone and Soft tissue COPY COPY107
-
Hepatobilliary29
