SBO causes
COMMON
- Adhesions (postoperative) 50–80%
- Hernias (external) 5–15%
- Malignancy (peritoneal) 5–15%
- Crohn’s disease <7%
OTHER
- Bowel wall lesions (causing intussusception)
- Intra-luminal mass: foreign body, gallstone ileus
- Extrinsic inflammatory lesions (appendiceal)
- Internal hernia
- Congenital malformation
- Superior Mesenteric Artery syndrom
Large Bowel Obstruction
Tumor (usually sigmoid carcinoma)
Volvulus (sigmoid, cecal)
Fecal impaction
Diverticulitis
Benign stricture (e.g. post-operative, inflammatory bowel disease)
Abscess
BO vs Ileus

Dysentry
Bacterial
- Gram positive – Clostridium Difficile
- Gram negative – Shigellosis, Enterohaemorrhagic E.coli, Salmonella, Yersinia enterocolitica
Protozoa
- Entamoeba histolytica
- Balantidium coli
Helminths
- Schistoma (S. mansion or S. japonicum)
- Ascariasis
- Trichuriasis
Non-infectious
- Inflammatory bowel disease
- Colorectal cancer
- Polyps
- Ischaemic colitis

Mackler’s Triad (oesophageal rupture)
- Chest pain
- Vomiting
- SC emphysema
Pathognomic for spontaneous oesophageal rupture - < 50% presentations
CXR oesophageal rupture
Abnormalities in up to 90% (none if early)
Pneumomediastinum
Right pl effusion - upper third rupture
Left pl effusion with distal third rupture
SC emphysema
Mediastinal widening
Pulmonary infiltrates
Oesophageal narrowings (4)
- C6 - cricopharyngeus muscle
- T4 - aortic arch
- T6 - bifurcation of trachea
- T11 - gastrooesophageal junction
Dysphagia - Neuromuscular
VASCULAR
- CVA
IMMUNOLOGICAL
- Dermatomyositis
- MS
- Myaesthenia gravis
- Polio
- Scleorderma
INFECTIOUS
- Botulism
- Diptheria
- Polio
- Rabies
- Sydenham’s chorea
- Tetanus
METABOLIC
- Lead poisoning
- Mg deficiency
OTHER
- Alzheinmer’s
- Amyotrophic lateral sclerosis
- Brain tunmour
- Depression
- Diabetic neuropathy
Dysphagia - Obstructive
- Aortic aneurysm
- Oesophageal dysmotility
- Oesophageal - rings, webs, stricture
- Oesophagitis
- FB
- Hypertrophic cervical spurs
- Mediastinal mass
- Left atrial enlargement
- Thyroid enlgargment
- Vascular anomalies
*
Dysphagia - other
- Alcoholism
- Decreased saliva production - Sjogren’s, radiation SE
- DM
- GORD
- Post-op
- Functional
Internal Hernia Locations
Haemorrhoid grades
- Painless, no prolapse
- Prolapse afters straining, spontaneous reduction
- Prolapse, require digital reduction
- Prolapse, irreducible
GI bleeding Risk Factors
- Medications
- Antiplatelets
- Anticoagulants
- NSAIDS
- Steroids
- PMHx
- PUD
- Chronix liver Dx
- Cirrosis
- Age >60yrs
- ETOH
- Smoker
- Comorbidities
- CCF
- DM
- Renal failure
- Malignancy
- AAA graft
UGI Bleed Mimics
- Epistaxis
- Hemoptysis
- Dental Bleeds
- Red Food Colouring
- Bismuth/Iron supplements
LGI bleed mimics
- Vaginal Bleeding
- Gross Hematuria
- Red Foods (BEETS)
Glasgow Blatchford Score
Screens need for intervention - Transfusion and OGD
NOT FOR VARICEAL BLEEDS
Score
0 - Rx as OP
1-6 - should have OGD within 24 hrs
Score >6 suggest high risk bleed and 50% need intervention
7-12 - MUST have OGD within 24 hrs
>12 - MUST have ODG within 12 hours
Must have OGD in 6 hours
* suspected variceal bleed
* Unstable
* High volume

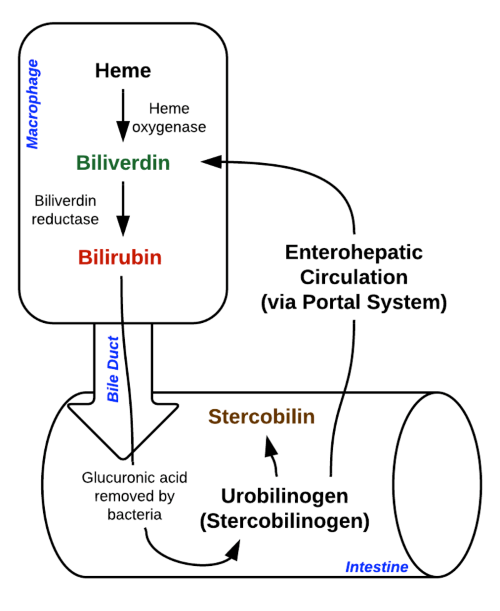
Jaundice differential
UNCONJUGATED HYPERBILIRUBINAEMIA
Pre-HEPATIC (overproduction of heme)
* Haemolysis - Haemolytic anaemias,
* Congenital - Gilberts, Crigler-Najar Syndrome
* Thalassaemia
* Trauma
* Severe CCF
* G6PD deficiency + oxidative drugs
HEPATIC (reduced hepatocyte Br uptake)
* Chronic hepatic cirrhosis
* Infection
* Viral / Bacterial / Protozoal
* Sepsis
* Drugs
* Toxins
* Alcohol
* Autoimmune
CONJUGATED HYPERBILIRIBUINAEMIA
POST-Hepatic (decreased excretion of Br)
* Hepatocellular (dec hepatocyte function)
* Hepatitis - viral, toxic, alcohol, AI
* Cirrhosis
* Drugs - paracetamol, methyldopa, pheyntoin
* Intra-hepatic
* Hepatitis
* Primary Biliary Cirrhosis
* Intrahepatic cholestasis
* Drugs - indomethacin, erythromycin, chlorproamzine, isoniazid, flucloxacillin, OCP
* Extra-hepatic
* Intraluminal - CBD stone, stenosis/ scarring PBC, PSC
* Pancreatitis
* External - Carcinoma - GB. pancreas, Ampullary
PREGNANCY
- Pre-eclampsia
- HELLP
- Acute fatty liver
- Hyperemesis gravidarum
- Cholestasis of pregnancy
Jaundice - Critical Causes
Hepatic
* Fulminant hepatic failure
* Toxin
* Viral
* Alcohol
* Ischaemic insult
* Reye’s syndrome
Biliary
* Ascending Cholangitis
Systemic
* Sepsis
* Heatstroke
Cardiovascular
* Obstructing AAA
* Budd Chiari
* Severe CCF
Haematological
* Transfusion reaction
OBS
* PET
* HELLP
* Acute fatty liver of pregnancy
* Cholestasis of pregnancy
Spontaneous Bacterial Peritonitis
Ascitic fluid infection without intra-abdominal surgically treatable source
Consider in Ascites + AP OR ascites + acute deterioration
+ve ascitic fluid bacterial culture + PMN count >250 cells/mm3
Cirrhosis or peritoneal dialysis patient (improper asepsis or contaminated dialysate)
Consider SBP versus secondary bacterial peritonitis
Orgs:
- E. coli
- Klebsiella
- Strep
- Enterococci
- Anaerobes
Rx
- Cextriaxone 2g IV
- If already on prophylaxis - Tazocin
SBP vs Secondary Bacterial Peritonitis
Ascitic fluid analysis
Spontaneous Bacterial Peritonitis
* No surgically treatable source
* Glucose <2.8mmol/L
* Serum protein-ascitic fluid gradient >1.1g/dL
* Total protein <1g/dL
* LDH not as high as bacterial
* Usually single organism
* No radiological abnormality
Bacterial peritonitis
* Surgically treatable source
* Glucose >2.8mmol/L
* Serum protein-ascitic fluid gradient <1.1g/dL
* Total protein >1g/dL
* LDH higher c.f. SBP
* Multiple organisms
* Radiology confirms obstruction, perforation, abscess
Hepatic Encephalopathy
State of cerebral and NM dysfunction secondary to increased ammonia levels
Severity doesn’t correltate well with ammonia level
Consider ppte - GI bleeding, infection, electrolyte disorder, dehrdration, constipation, RF, non-compliance with meds
Also consider DDx for AMS
Stages
- Stage I - apathy
- Stage II - lethargy + asterixis
- Stage III - stupor
- Stage IV - coma
Treatment
- Lactulose
- ABx - neomycin or metronidazole
Diarrhoea
TOXIN mediated - onset < 6hrs
- S. aureus - egg/mayo
- Bacillus cerues - fried rice
- E.colie - classic travellers diarrhoea
- Clostridium perfringens - meat/poultry
- Scombroid - dark meat fish - histamine
- Ciguatera - carvivorous fish - neuro
Invasive - delayed onset
- Salmonella - undercooked eggs/chicken
- Shigella - febrile - dysentry
- Campylobacter - chicken
- Yersinia - farm animals /chicken
Crohn’s vs UC

Pancreatitis Scoring Systems
Mortality from Pancreatitis
- Ranson’s
- Admission + 48hrs
- Glascow-Imrie
- 48 hrs post admission
- BISAP
- <48hrs




-
Resuscitation42
-
Cardiology102
-
Respiratory19
-
GI32
-
Neurology47
-
Endocrine25
-
Renal12
-
Toxicology82
-
Haem/Onc39
-
Administration29
-
Environment31
-
Paediatrics3
-
ENT26
-
Decision Rules10
-
Data Interpretation8
-
Radiology31
-
Trauma21
-
Differentials / Common Presentations1
-
Rheumatology18
-
ID44
-
O+G35
-
Eyes23
-
Calculations6
-
Signs/Symptoms7
-
Orthopaedics42
-
Max/Facs15
-
Difficult/Special Situations11
-
Renal / Urology5
-
STATs0
-
Psychiatry10
-
ACEM policies and procedures0
-
Drugs/Pharm10
-
Dermatology17
-
Metabolic13
