Spinal Shock
vs
Neurogenic Shock
Spinal Shock
Temporary loss of neurological function (spinal cord concussion) and automonic tone below level of spinal cord lesion
Typically <24hrs but can be days to weeks
Flaccid paralysis
Areflexia
Neurogenic shock
Distributive shock due to lack of sympathetic tone w/ injuries above T6
Bradycardia
Hypotension
Labile temperature - poikilothermia
Loss of bulbocavernosus reflex (involuntary contraction of internal anal sphincter when glans of penis or Foley catheter tugged)
Return of this indicated resolving spinal shock, otherwise

Wound Infection - Risk Factors
- Location - Leg>thigh>arms>feet>chest>back>face>scalp
- Open >8-12 hrs, Face>24hrs
- Contamination - devitalised tissue, foreing matter, saliva, stool
- Blunt / crush
- SC sutures
- Repair material - sutures > staples > tape
- LA with adrenaline
- High velocity missile injury
- Immunosupression - DM
Indications for Tetanus - booster / Ig
DTaP only
- Fully imunised and DTaP > 10yrs
- Fully immunised + DTaP < 5yrs + dirty wound / old
DTaP + TIG
- Not immunised
Refer these pts on to have full course with 2nd dose at 6 weeks and 3rd at 1yr
Wounds - ABx prophylaxis
- Bites
- Cat bites - all. (Staphylococcus, streptococcus and Pasturella multocida). Amox clav (875mg x 7d)
- Dog bites - controversial. Guidelines say limit to hand, very dirty, older patients, deep puncture and immunocompromised. Amox clav x7d
- Fight bites - human bites or assumed to the hand. First thoroughly look for tendon or joint damage. Streptococcus, staphylococcus, eikenella corrodens and bacteroides. Amox Clav , plastic surgery consultant opinion
- Intra-oral lacerations esp through-and-through
- Puncture wound of foot - no data supporting but should be considered especially in puncture through rubber shoe (pseudomonas). Ciproflox for pseudomonas, keflex for staph/strep. ?MRSA Septra or Doxycycline
- Delayed primary closure in high risk patient
- Open fractures / joints
- High velocity missile wounds
- Gross contamination / crush injury and immunospurresion
Parkland formula
TBSA (%) x wt x 3 - 4mL
1/2 fluid in first 8 hrs
1/2 fluid over next 16hrs
NB for kids add maintenance fluids
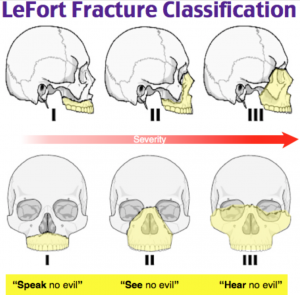
Le Fort Fractures
I - horizontal fractures of the maxilla that run above the teeth bearing alveolar process and the nasal f loor and hard palate
Separate teeth from upper face
II - pyramidal shaped extending from the upper nasal bridge at the apex, downwards through the medial wall of the orbits then on through the region of the zygomatico-maxillary suture lines.
Extend into orbital rim
III - extends through the upper nasal bridge, extend bilaterally across the orbits, to extend through the fronto-zygomatic sutures, then down through the zygomatic arches
Through orbital wall involving entire face
Unstable C-spine Injuries
C1
Jefferson
Posterior Neural arch
Atlanto-occipital dislocation
C2
Odontoid
Hangman’s fracture
Flexion-teardrop fracture
Extension tear-drop fracture (stable inflexion, unstable in extension
Bilateral facet dislocation
Spinal subluxation
Wedge fracture (if posterior column disrupted, >50% vertebral height or several #)
Stable C-Spine Injuries
Clay shoveler’s fracture (base spinous process, oblique)
Transverse process fracture
Unilateral facet dislocation
C-spine XR Rules
- Adequate views - C1-T1
- Alignment
- Ant Longitudinal Line
- Post Longitudinal Line
- Spinolaminal Line
- Spinour Process Line
- Bones
- Assess each vertebra for Fracture / Collapse / Avulsion
- Cartilage
- Soft tissue - Prevertebral ST swelling
- 6mm at C2 or 22mm at C6
- 6mm C2 or 14mm at C6 - kids
- Spaces
- Predental space - betw/ C1 tubercle and anterior face of dens
* <3mm adults
* <5mm children - Basion Dental interval
* <12mm XR
* <8.5mm CT - Power’s Ratio (atlanto-occipital dislocation
* AB/CD should be < 1 - Line of Swischuck - line from anterior aspect C1 to C3 spinous processes
* Anterior aspect of C2 should be < 2mm of this line
* Deviated > 2mm ? subluxation
* Deviated < 2mm ? pseudosubluxation
- Predental space - betw/ C1 tubercle and anterior face of dens
- Scan base skull, airway, sinuses
- AP and Odontoid views
[https://www.nyp.org/professionals/emergency-medicine/how-to-read-emergency-images/how-to-read-a-c-spine-film]
[https://dontforgetthebubbles.com/c-spine-x-ray-interpretation/
C-spine XR Rules - Odontoid view
Line 1
Lateral masses of C1 do not hang over lateral masses of C2
Line 2
No asymmetry of articular spaces between lateral masses of C1 and body C2
Line 3
No asymmetry between articular spaces of dens and C1
https://www.ebmconsult.com/articles/open-mouth-odontoid-radiograph
ASIA Impairment score
A = Complete
•no motor or sensory function below the lesion
B = Incomplete
•sensory but not motor function is preserved below the neurological level
C = Incomplete
•motor function preserved below the neurological level, with more than half of key muscles have a muscle grade < 3
D = Incomplete
•motor function preserved below the neurological level, and at least half of key muscles have a muscle grade of ≥ 3
E = Normal
•normal motor and sensory function
Extension vs Flexion Teardrop
Flexion
- Unstable 3 column
- Hyperflexion + axial load
- C5-6
- Assoc spinal cord injury - displaced posterior vert body into spinal canal
- Disrupted interspinous ligaments
- SURGERY
Extension
- Stable
- Hyperextension
- Usually C2
Trauma Laparotomy Indications
Immediate
- Evisceration
- Gunshot
- Penetrating injury - stab w/ breach of peritoneum
- Haemodynamic instability despite blood products
- Frank peritonism
- Free gas on imaging
- Ruptured diaphragm
Emergent
- Positive trauma USS
Blast injuries
- Primary - pressure effects - lung, ear, and gastrointestinal tract.
- Secondary – projectiles + penetrating injury
- Tertiary – when person is thrown through the air or effects due to wind i.e solid organ injury
- Quaternary – burns, asphyxia, toxic inhalants, psychological
Complications:
Lacerations, fractures, dislocations, crush injury, compartment syndrome, burns, DIC
Tip - if TM not ruptured then primary blast injury to other organs unlikely

Burns Referral Criteria
- Percentage
- Location
Escharatomy Indications
Ventilation
1. Inc airway pressures
2. Hypoxaemia
3. Difficulty ventilating
Circumferential Neck burns
Circumferential limb +
1. Decreased Doppler signal
2. Sats < 90% on affected limb
3. Pain. loss of senation or CRT > 2s = Early signs

Massive Haemothorax
Size:
Minimal < 350ml
- Small effusion erect CXR
Moderate 350-1500ml
- Visible erect CXR, diffuse opacity affected side
Massive > 1500ml
- ground glass appearance affected side supine
Clinical effects
1. Dec CO
2. Hypoventilation secondary to lung collapse
3. Dec preload via caval compression
Mx
1. Conservative for small
2. ICC for moderate/ massive
3. Thoracotomy
a. Stable > 200mls over 3hrs or >1.5L
b. Unstable > 100ml/hr or > 1L
Complications
Infection, bleeding
PTx
NV damage
Subdiaphragmatic placement
Cardiac injury (on left)
Tube misplacement
Insertion too far (common)
Causes severe pain if tube tip abuts on mediastinum
Haemodynamic compromise
- Hypotension can occur due to loss of tamponade effect, decreased intrathoracic pressure
- Try to maximise haemodynamics prior to ICC insertion whenever possible
Burns Chemical

Maxillofacial haemorrhage control
ETT to secure airway
C- Collar
Bite blocks
Bilateral nasal epistaxis catheters
REBOA
Insertion of endovascular balloon in the aorta to control haemorrhage and to augment afterload in traumatic arrest and haemorrhagic shock states
Indications
Age 18-69
PEA arrest < 10 mins + intrabdominal exanguination
SBP < 70
Contra-indications
Age >70y
Cardiac arrest from causes other then exanguination
PEA arrest >10 minutes
PEA arrest (<10 minutes) from exsanguination + femoral vessels not visible on USS
Aortic dissection
Pre-existing terminal illness or significant comorbidities
Endovascular balloons have been used to control haemorrhage in other settings such as aortic aneurysm surgery, gastro-intestinal bleeding, postpartum haemorrhage and trauma
ANATOMY of AORTA
Zone I = Left subclavian artery to the coeliac artery (approx 20cm)
Zone II = Coeliac artery to the most caudal renal artery (3cm long)
Zone III = most caudal renal artery to the aortic bifurcation (10cm long)
Skull fractures - Poor prognosis
Over vascular channel
Depressed
Diastatic (crosses suture lines)
Over MMA
Rhinorrhoea or ottorrhoea
-
Resuscitation42
-
Cardiology102
-
Respiratory19
-
GI32
-
Neurology47
-
Endocrine25
-
Renal12
-
Toxicology82
-
Haem/Onc39
-
Administration29
-
Environment31
-
Paediatrics3
-
ENT26
-
Decision Rules10
-
Data Interpretation8
-
Radiology31
-
Trauma21
-
Differentials / Common Presentations1
-
Rheumatology18
-
ID44
-
O+G35
-
Eyes23
-
Calculations6
-
Signs/Symptoms7
-
Orthopaedics42
-
Max/Facs15
-
Difficult/Special Situations11
-
Renal / Urology5
-
STATs0
-
Psychiatry10
-
ACEM policies and procedures0
-
Drugs/Pharm10
-
Dermatology17
-
Metabolic13
