Malaria
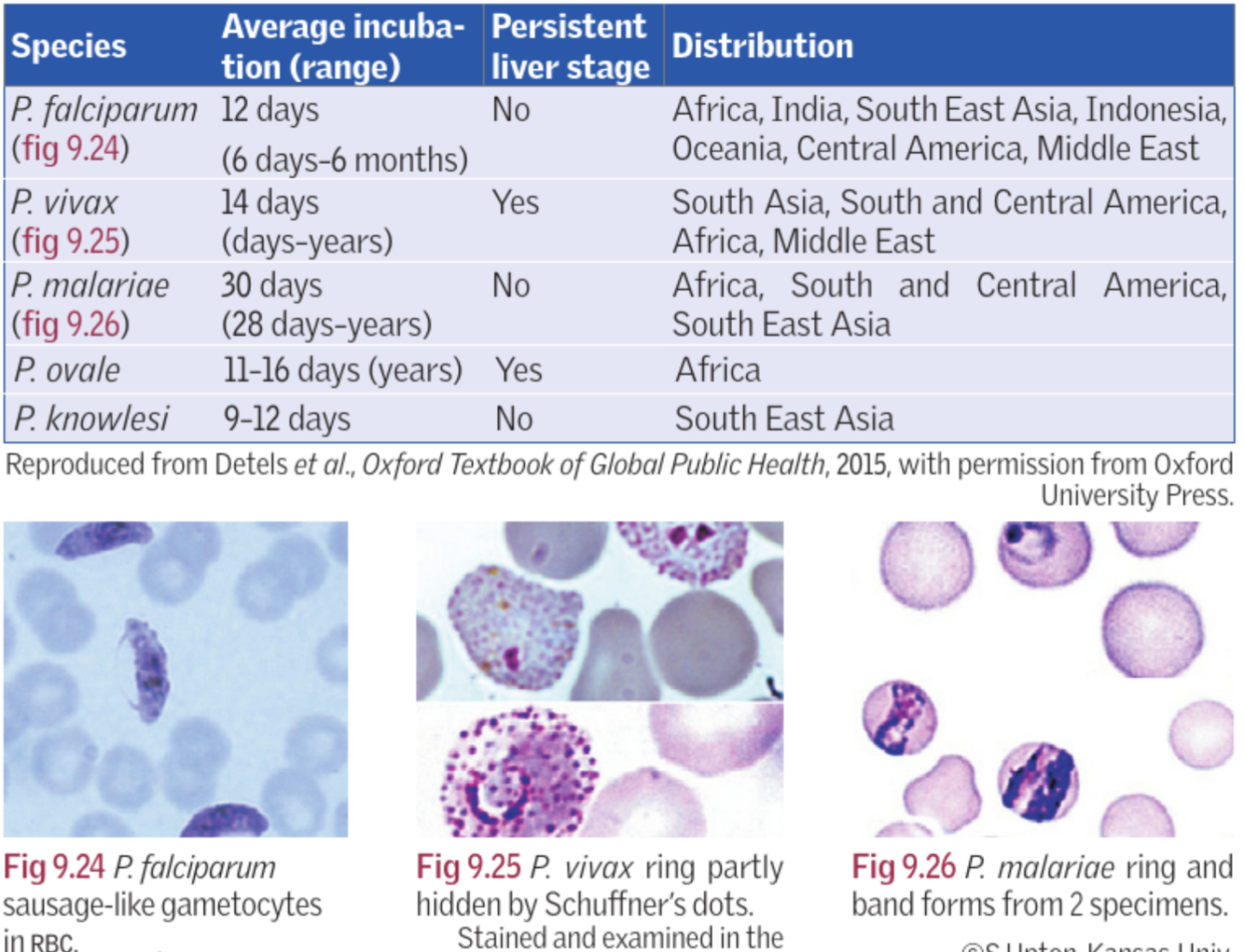
- What are the five main species of plasmodium?
- Symptoms?
- o/e
- Ix:
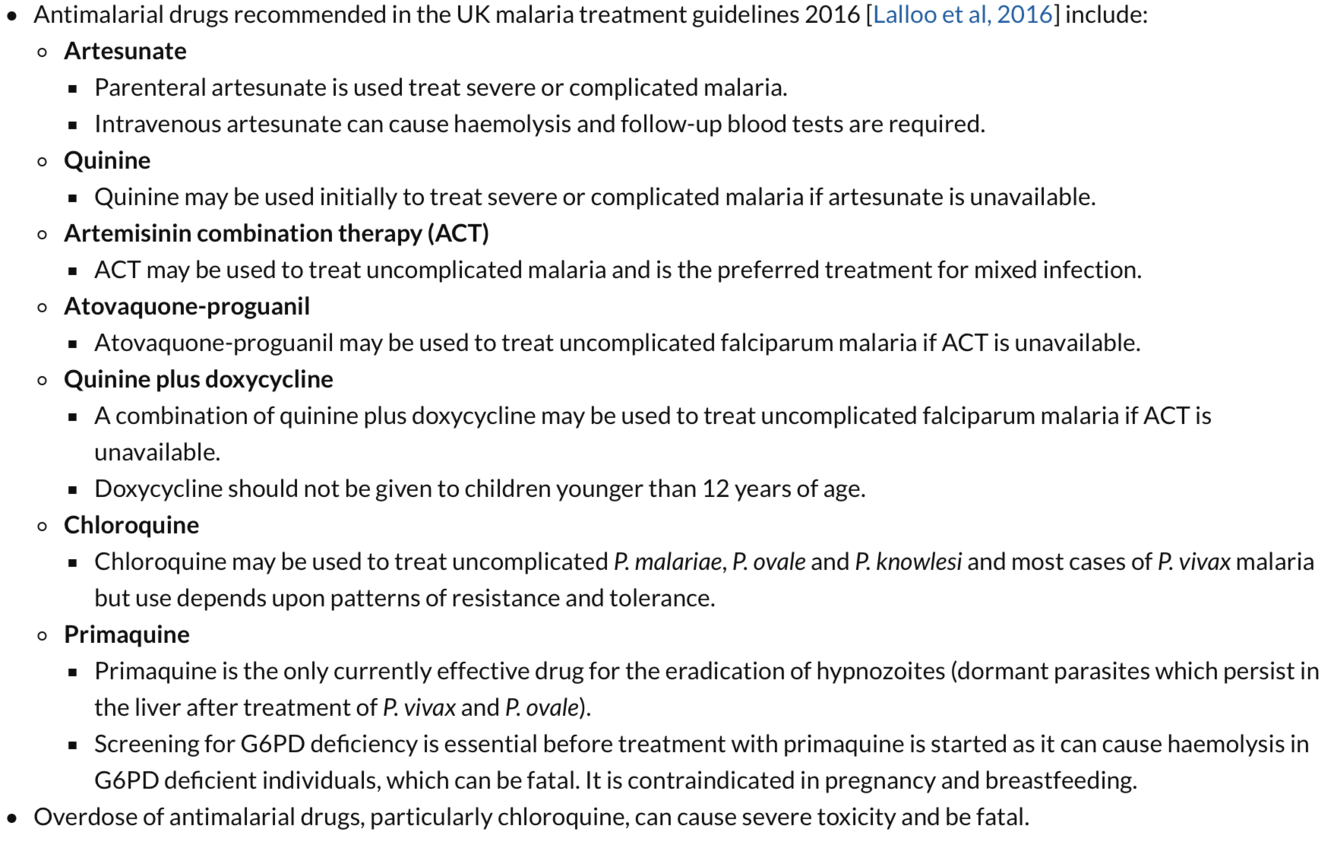
- Rx
- Untreated P. falciparum infection can cause
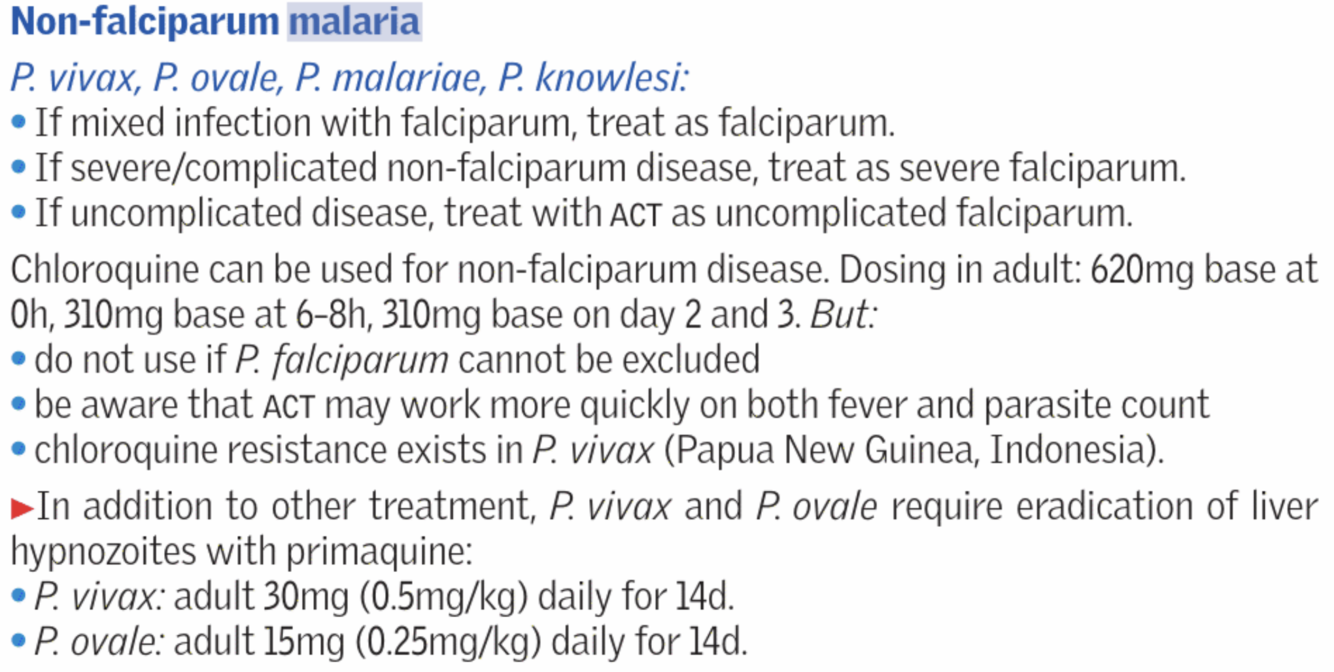
- Features of non falciparum
- Ovale and vivax
- DD
1.
- falciparum ~ usually Africa
- vivax ~ india
- ovale~ india
- malariae
- knowlesii
- Abrupt onset of rigors followed by high fevers, malaise, severe headache and myalgia, vague abdominal pain, N+V, diarrhoea (25%)
- Jaundice and hepatosplenomegaly
4.
Blood film x3 (if falciparum % of parasitised cells should be given >2% chance if being severe, >10% severe)
FBC (anaemia, thrombocytopenia, leukopenia), U&Es, LFTs (abnormal), glucose, coagulation
Head CT scan if neurological symptoms
CXR
5.
P. falciparum:
1st line: Artesunate
2nd line: Quinine + doxycycline
P. vivax, ovale,malariae:
• Chloroquine
• Dormant hypnozoites (liver)
– Can recur months-years later
– Give additional primaquine
- hypoglycemia, renal failure, pulmonary edema, and neurologic deterioration, leading to death
- fever, headache, splenomegaly
Plasmodium vivax/ovale: cyclical fever every 48 hours.
Plasmodium malariae: cyclical fever every 72 hours
Plasmodium malariae: is associated with nephrotic syndrome.
- ? malaria have a hypnozoite stage and may therefore relapsefollowing treatment.
- Dengue, typhoid, hepatitis
State some antimalarial prohphylaxis regimens?
prophylaxis does not prevent all malaria

What do each of the plasmodiums look like on a blood film?
what is their incubation periods?
Features of severe falciparum infection.
How to treat uncolplicated falciparum infection
impaired conciousness, schizonts
artemethur lumefantrime + fatty meal
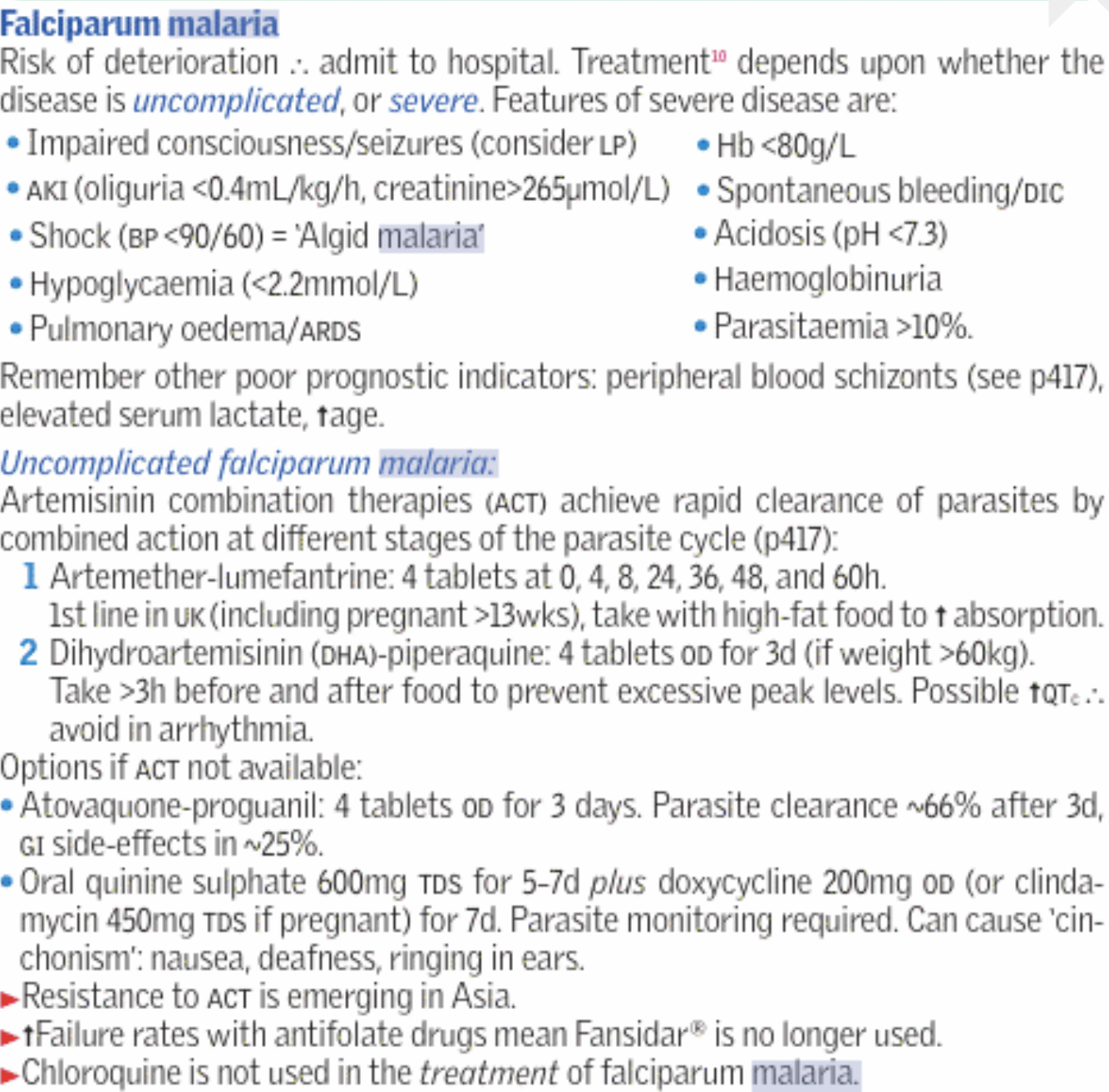
How to treat complicated malaria infection
Artesunate (5days)
then full course of Artemesinin combination therapies (artemether - lumefantrine)
How to treat non falciparum malaria
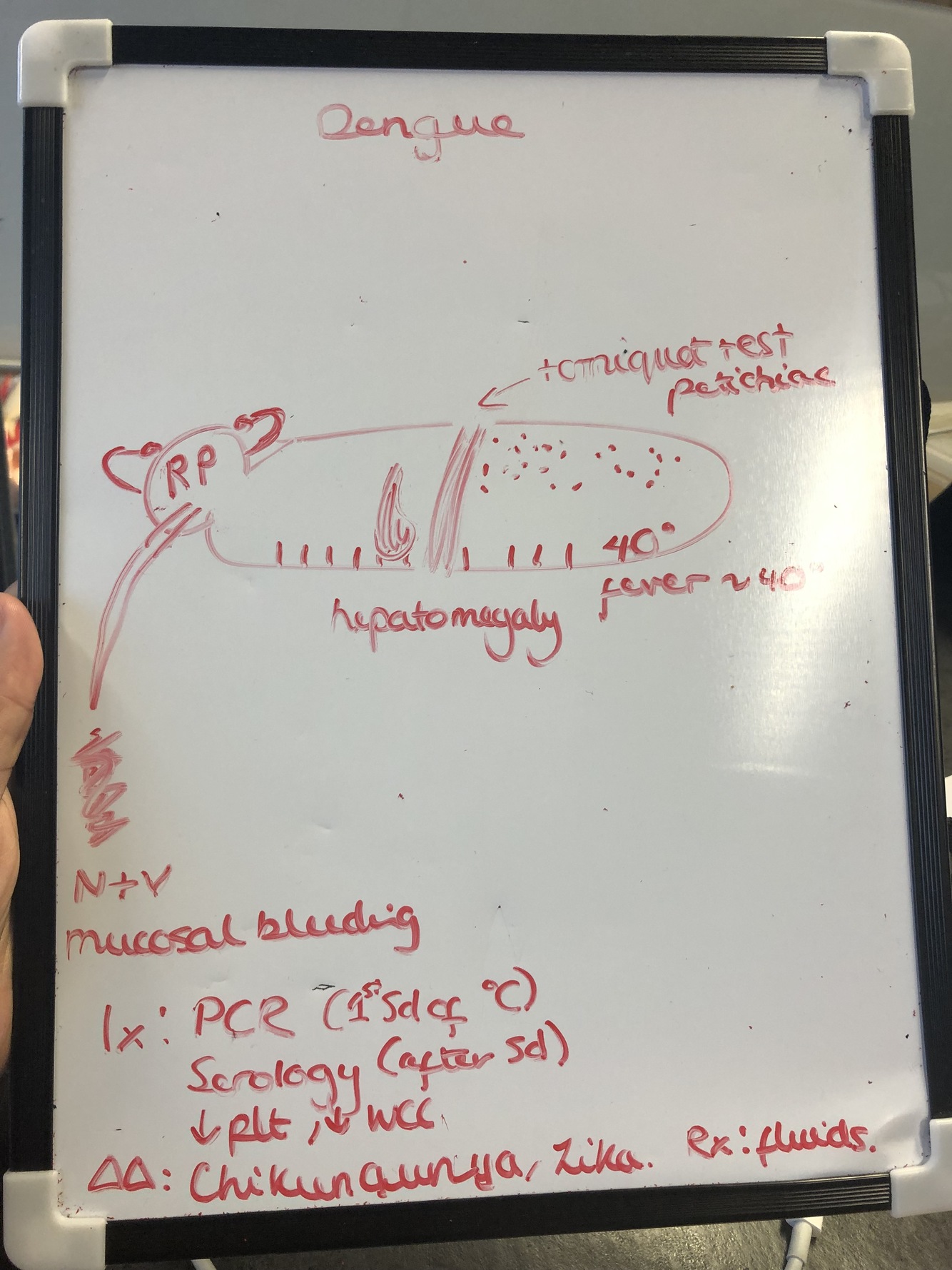
Dengue
sign/symp
Ix
DD
Rx
retro orbital pain
headache
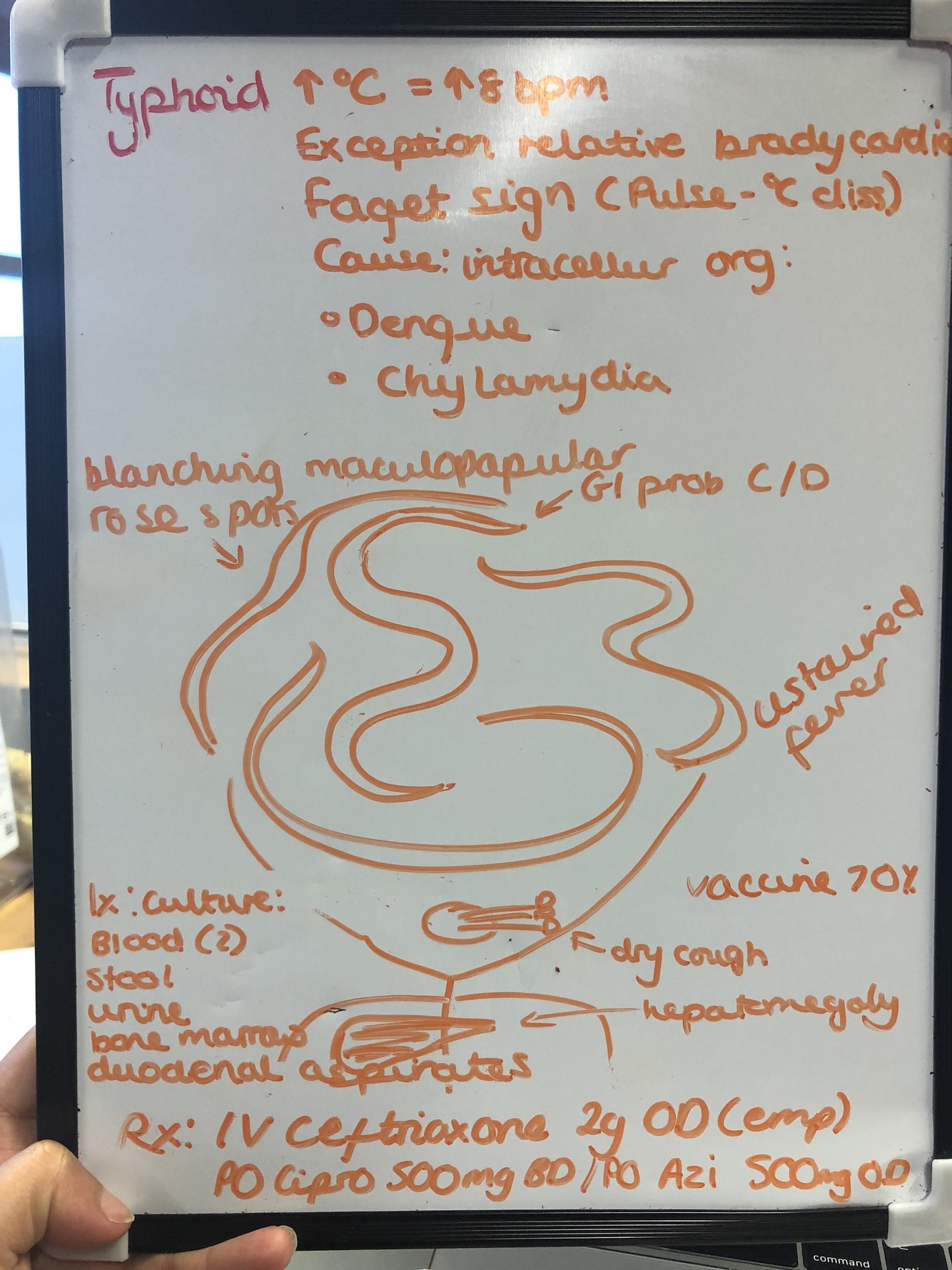
Typhoid fever
symptoms/signs
Ix
Rx
Cause: ~ salmonella enterica (bacterium)
Spread: FO route (Food/water)
Incubation: 3-21 days
Signs and symptoms:
Week 1: Bradycardia, epistaxis (25%), leukopenia, eosinopenia, lymphocytosis
Week 2: 40 °C, bradycardia (sphygmothermic dissociation or Faget sign), Rose spots, Rhonchi (rattling breathing sounds), Widal test is strongly positive, with antiO and antiH antibodies
Week 3 complications:
Intestinal haemorrhages
Perforation in distal ileum
Encephalitis
Ix:
Cultures (blood, bone marrow or stool)
Widal test (antibodies against Salmonella antigens O-somatic and H-flagellar)
Bloods: FBC (leukopenia)
Ix to rule out malaria and other causes
Pyrexia of unknown origin (most resolve within 4wks)
- Classical definition:
- Common causes:
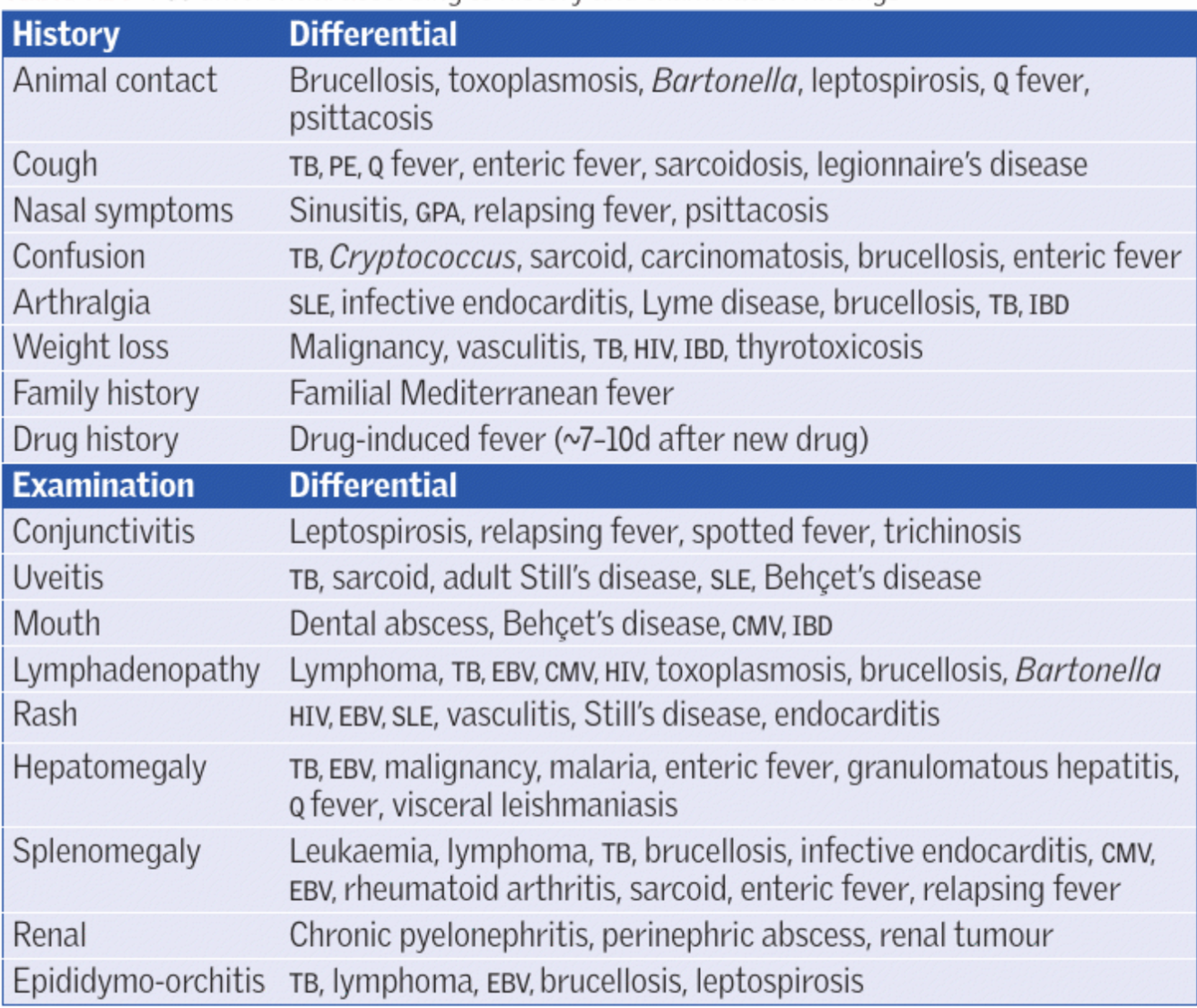
- History:
- Examination:
- Ix
- Management points:

- Temperature > 38 degrees on multiple occasions
- Illness of >3 wks duration
- No diagnosis despite >1 wk’s worth of inpatient Ix
- Temperature > 38 degrees on multiple occasions
- Infective – TB, abscesses, IE, brucellosis
AI/CT – adult onset Still’s disease, temporal arteritis, granulomatosis with polyangitis (Wegener’s granulomatosis)
Neoplastic – leukaemias, lymphomas, renal cell carcinoma
Other – drugs, thromboembolism, hyperthyroidism, adrenal insufficiency
- Chronology of symptoms? Pets/animal exposure?Travel?Occupation?Medications?Family history?Vaccination history?Sexual contacts?
- Lymph nodes, stigmata of endocarditis, evidence of weight loss, joint abnormalities
5.
Blood: FBC/U+Es/LFTs/bone profile/CRP/clotting, TFTs,multiplesets of blood cultures, LDH, ferritin, B12, folate, immunoglobulins*, autoimmune screen* (RF, ANA, dsDNA, pANCA, cANCA, C3, C4)
Micro/virology: HIV, Hepatitis B+C, syphilis, MSU, sputum cultures, malaria films*, atypical pneumonia screen*, viral swabs, CMV+EBV serology, Brucella serology*, Coxiella serology*, ASO titre*, fungal serology/PCR*
Imaging: CXR, CT thorax/abdomen/pelvis, transthoracic echo, MR head*, MR spine*, radiolabelled white cell scans*, PET scan*
Biopsies*: MC+S, TB culture, histology on all samples. Sites: Bone marrow, lymph nodes, abscesses, liver
* = not all patients need this test – check before requesting it.
- Aim to establish the diagnosis, rather than treating blindly
- Do NOT start empirical antibiotics/steroids/antifungals without speaking to a registrar/consultant
- We often ask rheumatology and haematology to see PUO patients, depending on the presentation.
- Try and stay up to date on what tests have been done – a front sheet for the notes is very helpful
- Stable patients can be managed as outpatients following a period of observation in hospital
- In patients with no diagnosis despite prolonged investigation, the prognosis tends to be good
- Aim to establish the diagnosis, rather than treating blindly
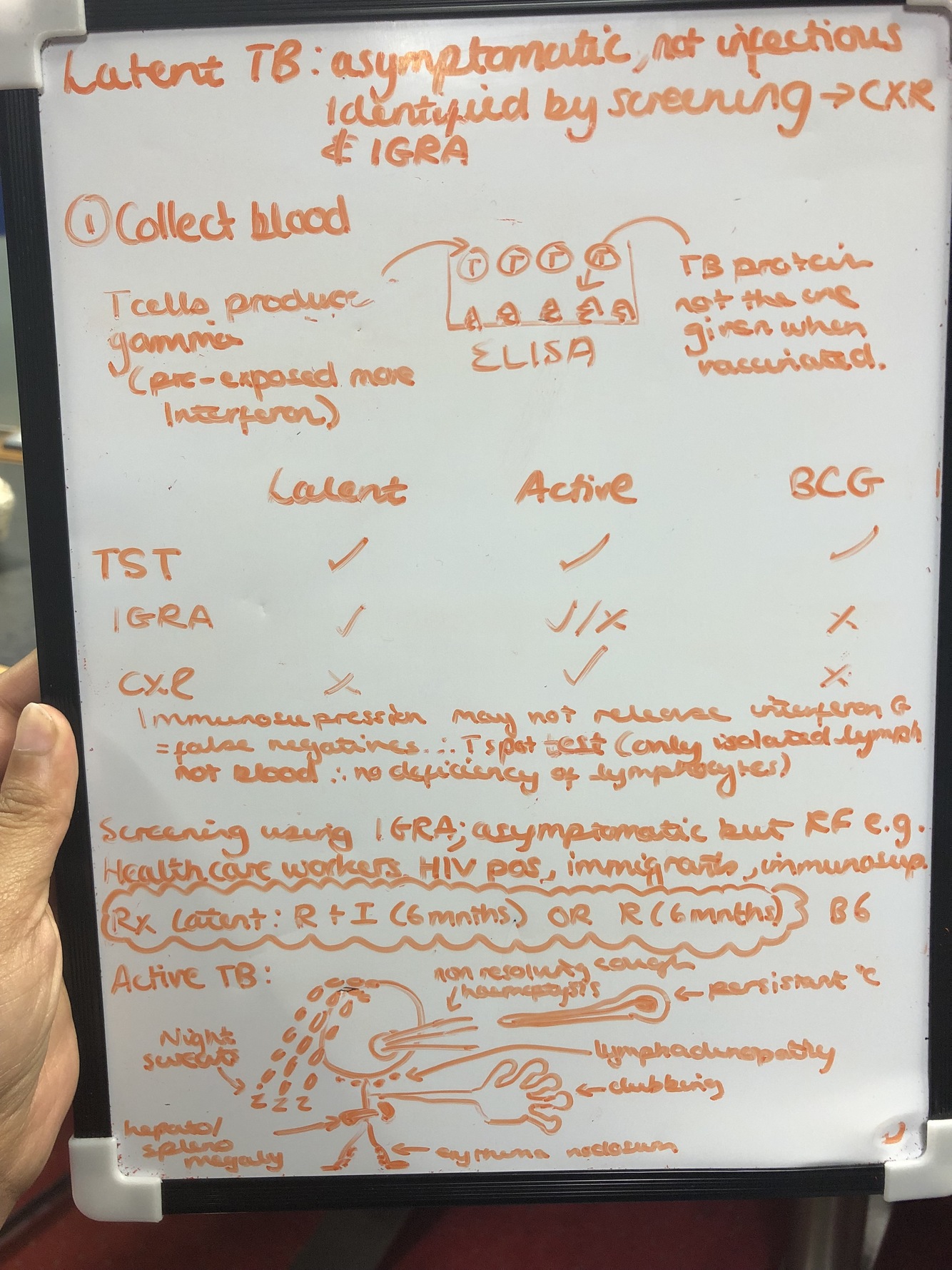
- Define latent tb
- Describe the IGRA test
- State all the Tb test and which forms of tb will show a positive and negative result
- who do we screen
5. How do you treat latent tb
6. signs of active tb?
- 6 months of rifamipicin
Ziehl Neelson stain
- Active TB Ix
2. Paradoxical reaction: steroids
Imaging
CXR: Mediastinal lymphadenopathy, cavitating pneumonia, pleural effusion
CT: Lymphadenopathy. Nodes with central necrosis are more suggestive. Lesions in viscera can also be seen
MRI: leptomeningeal enhancement in TB meningitis
Biopsy/samples:
Culturing (up to 6wks) the bacteria is the gold standard for diagnosis
Pulmonary TB– sometimes can be identfied from sputum samples or induced sputum (sputum taken after a nebuliser of 7% hypertonic saline).
- If TB can be seen on a sample using simple microscopy it is said to be ‘smear positive’. This implies a high bacterial load and high infectivity. ATT can be started immediately as there is a high chance it will culture.
- If a sputum sample is ‘smear negative’ then we usually proceed to bronchoscopy +/- EBUS (endobronchial ultrasound guided biopsy) of pulmonary lymph nodes. Once these samples are taken we start ATT
Meningeal TB– lumbar puncture for TB culture and TB PCR
Lymph node TB - core biopsy of lymph node (FNA is not adequate)
Pericardial TB– ideally pericardiocentesis – often not practical
Gastrointestinal– colonoscopy and bowel biopsy/ Ultrasound guided omentum biopsy
Histology: Caseating/necrotising granulomatous inflammation
- Inc in inflammation as bacteria die causing worsening symptoms. Usually occurs at the start of treatment
If TB is affecting sites where additional swelling cannot be tolerated (e.g. meningeal/spinal/pericardial TB) then steroids are given at the start of treatment

- Special consideration tb:
- Treatment for active tb
s/e
- Monitoring:
- Contact Tracing
TB meningitis/CNS TB:
- 1% meninges affected. All pts with military TB should have a LP to exclude TB meningitis
- symptoms varied:
Initially subtle: personality change and headache
meningitic
finally comatose over several weeks
more insidious onset than viral/bacterial meningitis
- MRI: leptomeningeal enhancement
- LP: high protein, low glucose, lymphocytosis
Significance: If a patient has TB meningitis then the paradoxical reaction to ATT can be fatal. They are therefore given steroids when starting treatment. The treatment is also longer (12 months).
Pericardial TB:
- pericardial effusion, tamponade
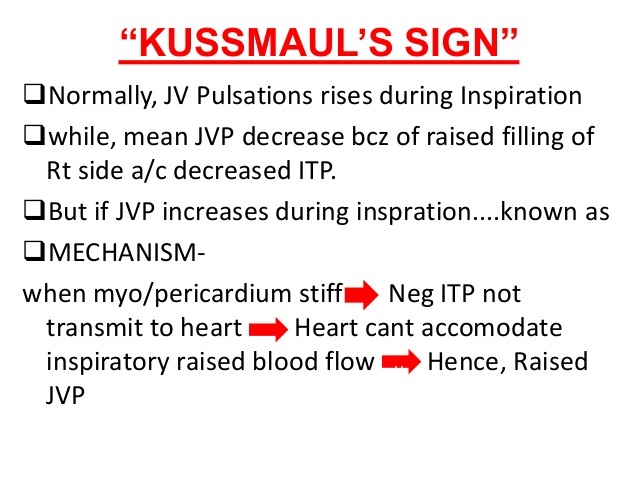
Signs: pericardial rub or kussmaul’s sign. Paradoxical reaction can result in tamponade.
- Duration of treatment is 6 months. Steroids are given at the start of treatment
Disseminated/Miliary TB
- widespread: CNS/bone marrow/pericardium.
- All should have neuroimaging (CT/MRI head) +/- lumbar puncture to exclude CNS involvement.
- Treatment shouldn’t be delayed whilst awaiting biopsies (ATT is usually started as soon as it is determined whether or not there is CNS involvement)
MDR and non-MDR resistant TB
- Consider in patients who have had incomplete Rx for TB previously
- Usually seen in patients from abroad
- Treatment is specialised and is based on sensitivities. Treatment regimen is usually decided by consultant
- Infection control is paramount: negative pressure room & staff should wear masks/PPE
2.
2 months (intensive phase):
- Rifampicin + Isoniazid + Pyrazinamide + Ethambutol = RIFATER
- pyridoxine (vitamin b)
Then 4 months (continuation phase):
- Rifampicinand isoniazid = RIFINAH
- pyridoxine
Rifampicin
- urine/tears to turn orange (reverses when rifampicin stops)
- Drug induced hepatitis +
Isoniazid
- Peripheral neuropathy (reduced by giving pyridoxine)
- Colour blindness
- Drug induced hepatitis ++
Pyrazinamide
- Drug induced hepatitis +++
Ethambutol
- optic neuropathy/ reduced visual acuity
3.
Before treatment: baseline LFT and visual acuity (if using ethambutol)
During treatment: monitor LFTS
If LFTS derange Rx can either be stopped and the drugs gradually reintroduced once they have normalised
or a “liver friendly” regimen can be given (e.g. amikacin, levofloxacin & ethambutol) but the treatment duration is longer (up to 24 months)
- referred to the TB nurses
perform contact tracing and will test household contacts with either CXR or QuantiFERON testing and will treat any latent TB
Usually if household contacts were going to catch TB it would be before the patient was admitted so visitors are allowed – unless they have resistant TB
Infection control
- Patients with non-resistant pulmonary TB should be nursed in a side room.
- After 2 weeks of treatment patients are generally considered non-infectious to immunocompetent individuals.
- If the ward also manages immunocompromised patients, including HIV (i.e our ward!) then patients with respiratory TB need to be nursed in a side room until discharge regardless of whether they are smear positive or negative (there are criteria by which they can come out but they are very stringent)
- Smear positive patients can still be discharged home but would need to quarantine themselves at home until they have completed 2 weeks of treatment.
- NICE guidance is that staff do NOT need to wear masks/aprons unless MDR TB is suspectedor they are performing an aerosol generating proceduresuch as giving a nebuliser.
- Patients with smear positive TB DO need to wear a mask when leaving their roomuntil they have completed 2 weeks of treatment.
Go and complete session 9 repro!!!
Post-exposure prophylaxis for HIV: oral antiretroviral therapy for 4 weeks
patchy opacities in the right apex and bilateral hilar enlargement: The feature of profound desaturation on exercise however is a very common clinical feature in PCP and this is the key feature of the history and examination which gives the answer in this case.
sputum often fails to show PCP, bronchoalveolar lavage (BAL) often needed to demonstrate PCP (silver stain shows characteristic cysts)
Management?
- what is the first line abx in nuetropenuc sepsis?
- co-trimoxazole
- IV pentamidine in severe cases
- steroids if hypoxic (if pO2 < 9.3kPa then steroids reduce risk of respiratory failure by 50% and death by a third)
- Tazocin is recommend as the first-line antibiotic by NICE
Lyme disease is caused by the spirochaete Borrelia burgdorferi and is spread by ticks.
Features
- early: erythema chronicum migrans (‘bulls-eye’) rash is seen in around 80%. Systemic features include fever, arthralgia
- cardiovascular: heart block, myocarditis
- neurological: facial nerve palsy, meningitis
Investigation
- NICE recommend that Lyme disease can be diagnosed clinically if erythema migrans is present
- enzyme-linked immunosorbent assay (ELISA) antibodies to Borrelia burgdorferi are the first-line test
- if this test is positive or equivocal then an immunoblot test for Lyme disease should be done
Management of suspected/confirmed Lyme disease
- doxycycline if early disease. Amoxicillin is an alternative if doxycycline is contraindicated (e.g. pregnancy)
- ceftriaxone if disseminated disease
- Jarisch-Herxheimer reaction is sometimes seen after initiating therapy: fever, rash, tachycardia after first dose of antibiotic (more commonly seen in syphilis, another spirochaetal disease)
Hepatitis C
patitis C is likely to become a significant public health problem in the UK in the next decade. It is thought around 200,000 people are chronically infected with the virus. At risk groups include intravenous drug users and patients who received a blood transfusion prior to 1991 (e.g. haemophiliacs).
Pathophysiology
hepatitis C is a RNA flavivirus
incubation period: 6-9 weeks
Transmission
the risk of transmission during a needle stick injury is about 2%
the vertical transmission rate from mother to child is about 6%. The risk is higher if there is coexistent HIV
breast feeding is not contraindicated in mothers with hepatitis C
the risk of transmitting the virus during sexual intercourse is probably less than 5%
there is no vaccine for hepatitis C
After exposure to the hepatitis C virus only around 30% of patients will develop features such as:
a transient rise in serum aminotransferases / jaundice
fatigue
arthralgia
Investigations
HCV RNA is the investigation of choice to diagnose acute infection
whilst patients will eventually develop anti-HCV antibodies it should be remembered that patients who spontaneously clear the virus will continue to have anti-HCV antibodies
Outcome
around 15-45% of patients will clear the virus after an acute infection (depending on their age and underlying health) and hence the majority (55-85%) will develop chronic hepatitis C
Chronic hepatitis C
Chronic hepatitis C may be defined as the persistence of HCV RNA in the blood for 6 months.
Potential complications of chronic hepatitis C
rheumatological problems: arthralgia, arthritis
eye problems: Sjogren’s syndrome
cirrhosis (5-20% of those with chronic disease)
hepatocellular cancer
cryoglobulinaemia: typically type II (mixed monoclonal and polyclonal)
porphyria cutanea tarda (PCT): it is increasingly recognised that PCT may develop in patients with hepatitis C, especially if there are other factors such as alcohol abuse
membranoproliferative glomerulonephritis
Management of chronic infection
treatment depends on the viral genotype - this should be tested prior to treatment
the management of hepatitis C has advanced rapidly in recent years resulting in clearance rates of around 95%. Interferon based treatments are no longer recommended
the aim of treatment is sustained virological response (SVR), defined as undetectable serum HCV RNA six months after the end of therapy
currently a combination of protease inhibitors (e.g. daclatasvir + sofosbuvir or sofosbuvir + simeprevir) with or without ribavirin are used
Complications of treatment
ribavirin - side-effects: haemolytic anaemia, cough. Women should not become pregnant within 6 months of stopping ribavirin as it is teratogenic
interferon alpha - side-effects: flu-like symptoms, depression, fatigue, leukopenia, thrombocytopenia
c diff
Clostridium difficile
Clostridium difficile is a Gram positive rod often encountered in hospital practice. It produces an exotoxin which causes intestinal damage leading to a syndrome called pseudomembranous colitis. Clostridium difficile develops when the normal gut flora are suppressed by broad-spectrum antibiotics. Clindamycin is historically associated with causing Clostridium difficilebut the aetiology has evolved significantly over the past 10 years. Second and third generation cephalosporins are now the leading cause of Clostridium difficile.
Other than antibiotics, risk factors include:
proton pump inhibitors
Features
diarrhoea
abdominal pain
a raised white blood cell count is characteristic
if severe toxic megacolon may develop
Diagnosis is made by detecting Clostridium difficile toxin (CDT) in the stool
Management
first-line therapy is oral metronidazole for 10-14 days
if severe or not responding to metronidazole then oral vancomycin may be used
fidaxomicin may also be used for patients who are not responding , particularly those with multiple co-morbidities
for life-threatening infections a combination of oral vancomycin and intravenous metronidazole should be used
stop opiods/anti motility - inc risk of toxic megacolon
Other therapies
bezlotoxumab is a monoclonal antibody which targets Clostridium difficile toxin B - it is not in widespread use
Chronic HIV-associated nephropathy will have large/normal sized kidneys on ultrasound whereas most patients with chronic kidney disease have bilateral small kidneys.
Other conditions that can cause enlarged kidneys on ultrasound include:
autosomal dominant polycystic kidney disease, diabetic nephropathy and amyloidosis.
-
Orthopaedics - Clinical conditions49
-
Drugs57
-
Pain management1
-
DVT assessment & management15
-
Care of the diabetic surgical patient and the surgical patient on steroids.38
-
peri operative42
-
peri op (general)18
-
Period Cardioresp8
-
General surgery43
-
GP day cases55
-
Medicine day case23
-
Hepato pancreatic biliary surgery7
-
contraception10
-
Rheumatology56
-
Paediatrics35
-
geri27
-
Urology10
-
Vascular surgery17
-
ID19
-
Renal workbook21
-
surgery workbook16
