RCC
- E
- Other renal malignancies include:
- Pathophysiology
- RF
- CF
- Paraneoplastic syndromes
- DD
- Ix
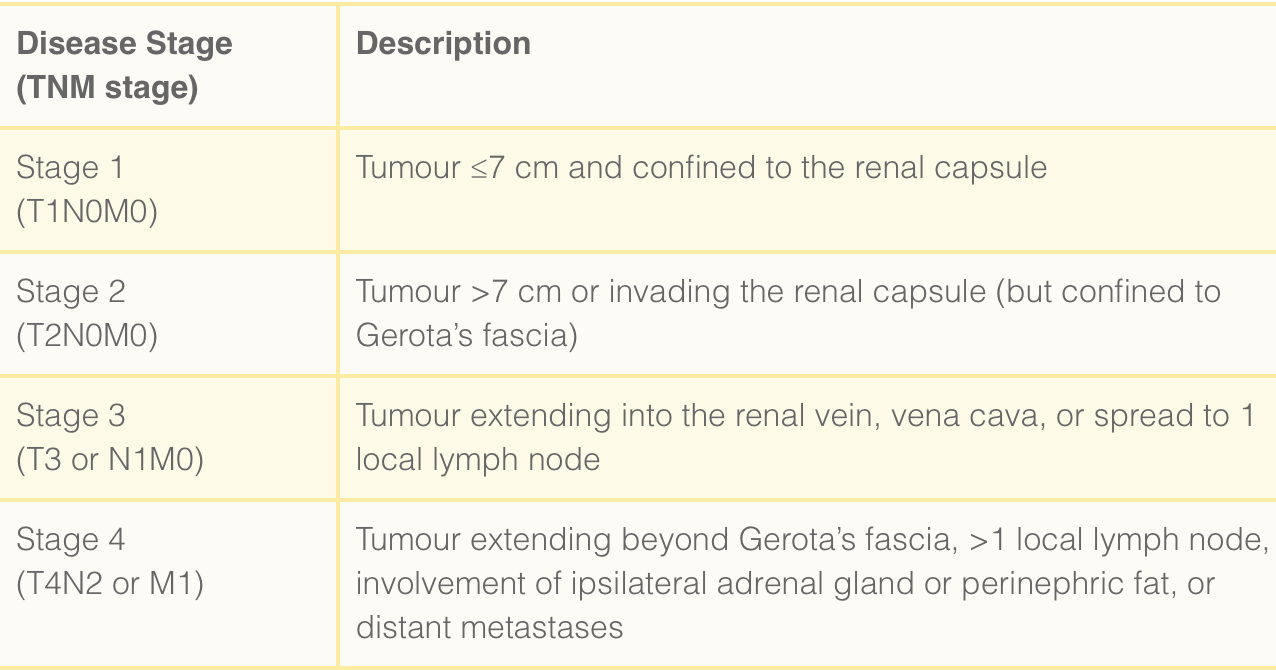
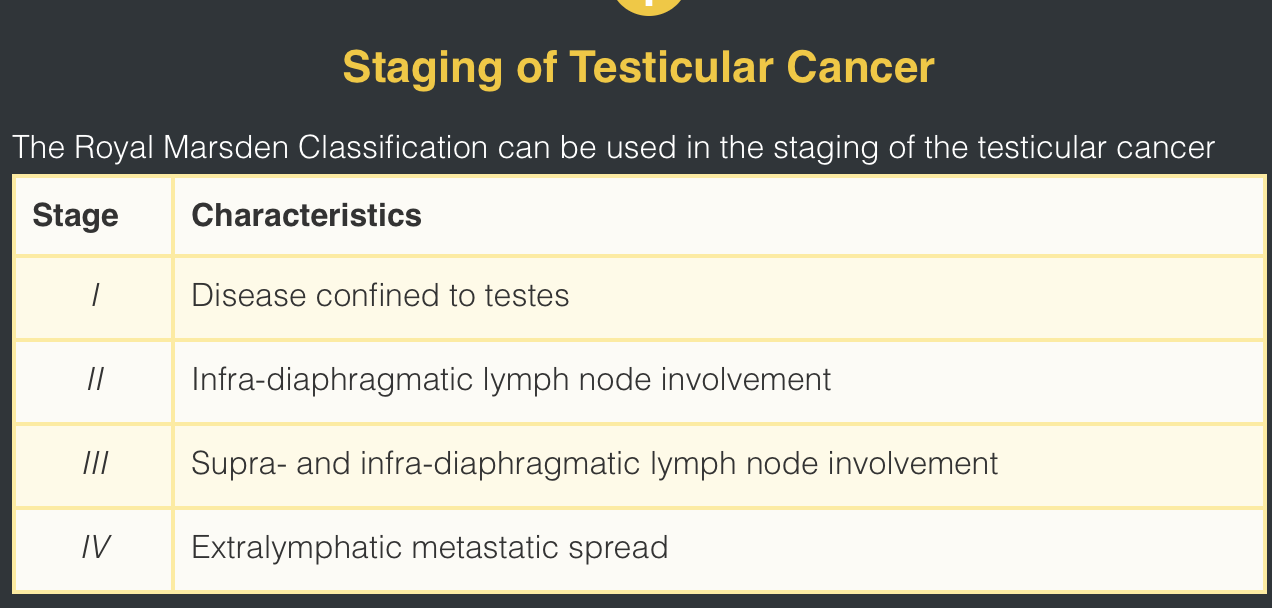
- stage
- Rx
- 1.5xmen
peak incidence 50-70yrs
- transitional cell carcinoma (urothelial tumours),
nephroblastoma in children (Wilm’s tumour),
squamous cell carcinomas (chronic inflammation secondary to renal calculi, infection and schistosomiasis).
- adenocarcinoma of the renal cortex
~upper pole
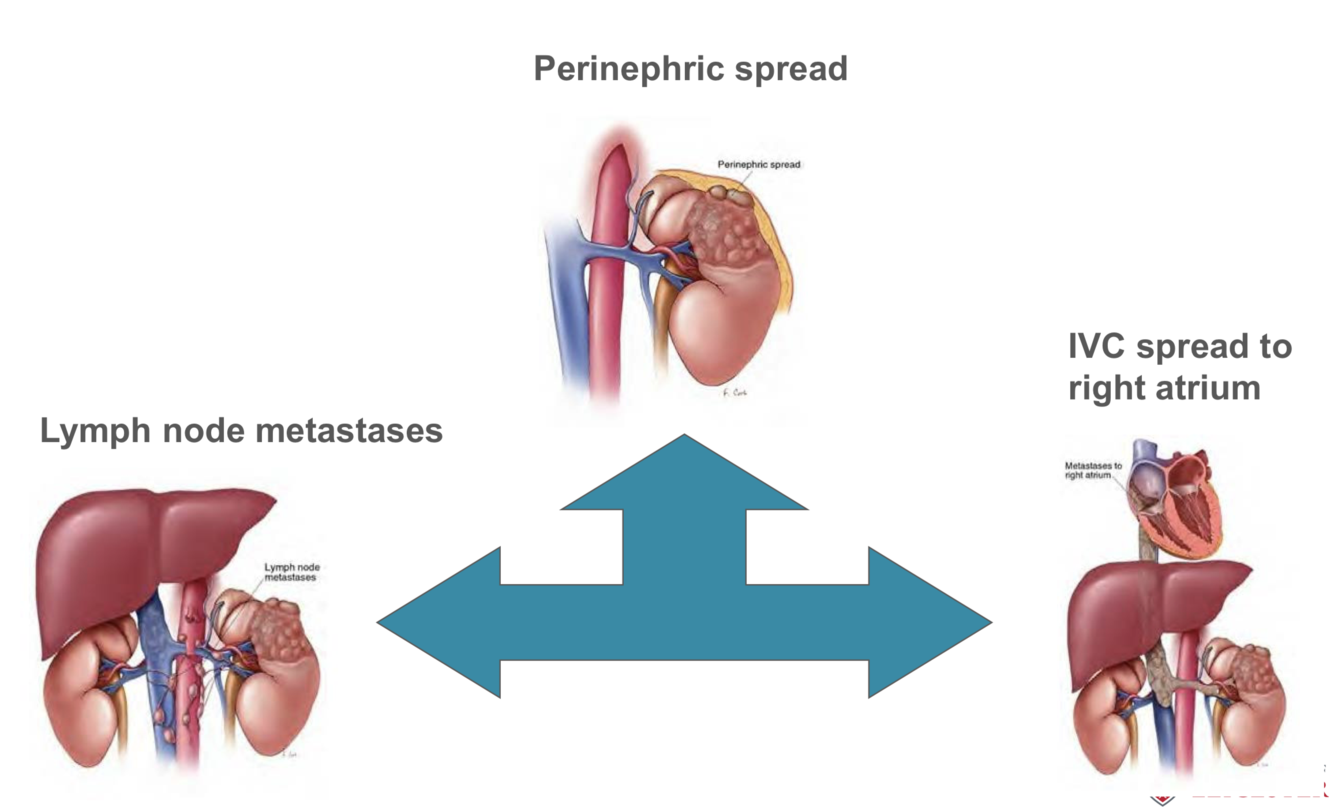
direct invasion: perinephric tissues, adrenal gland, renal vein* or the inferior vena cava
lymphatic system: pre-aortic and hilar nodes
haematogenous spread: bones, liver, brain and lung
4.
- smoking 2x
- industrial exposure to carcinogens (such as cadmium, lead, or aromatic hydrocarbons)
- dialysis (30x increase); hypertension; obesity, and anatomical abnormalities such as polycystic kidneys and horseshoe kidneys.
- Hippel-Lindau disease (associated with bilateral multifocal toumours), BAP1 mutant disease, and Birt-Hogg-Dube syndrome.
5.
- incidentally on abdominal imaging (50%)
- haematuria, either visible or non-visible
- flank pain, flank mass
o/e:
- left varicocoele, due to compression of the left testicular vein as it joins the left renal vein
- palpated in the flank
- lethargy or wt loss
- ectopic secretion of hormones by RCC:
- polycythaemia due to erythropoetin,
- hypercalcaemia due to PTH,
- HTN due to renin,
- or pyrexia of unknown origin,
- or with the clinical features of metastasis (such as haemoptysis or pathological fractures)
- urological malignancy, renal stones, or urinary tract infection
8.
- bloods: FBC, U&E, calcium, liver function tests and C-reactive protein.
- Urinalysis should be formed for evidence of non-visible haematuria and urine should be sent for cytology.
Imaging
- CT imaging of the abdomen-pelvis pre and post IV contrast is the gold standard
- USS
Special
biopsy
- image
10.
Localised Disease
surgical (laparoscopic or open approaches)
Smaller tumours, a partial nephrectomy
larger tumours, a radical nephrectomy (remove the kidney*, perinephric fat, and local lymph nodes en bloc)
Not fit for surgery percutaneous radiofrequency ablation or laparoscopic/ percutaneous cryotherapy
Renal artery embolisation may be required for haemorrhaging disease, prior to any radiofrequency ablation, or for unresectable palliative cases.
Surveillance of slow growing small renal masses can be employed in patients unfit or unwilling to undergo surgery with a limited life expectancy
*The adrenal gland should be spared if possible, except in cases of large upper pole tumours which have a high risk of adrenal invasion
Metastatic Disease (Chemotherapy iineffective)
Fit: nephrectomy + immunotherapy (such as IFN-α or IL-2 agents)
Biological agents (combination): Sunitinib (a tyrosine kinase inhibitor) and Pazopanib (also a tyrosine kinase inhibitor)
Metastasectomy (surgical resection of solitary metastases) is recommended where the disease is resectable and the patient is otherwise well.
25% have metastasis at presentation. Survival for patients who have undergone nephrectomy is around 70% at 3 years and 60% at 5 years, however those with worse stage disease have a poorer prognosis.
PROSTATE CANCER\
- Prostate adenocarcinomas can be categorised into two types:
- RF
- cf
- DD
- Ix
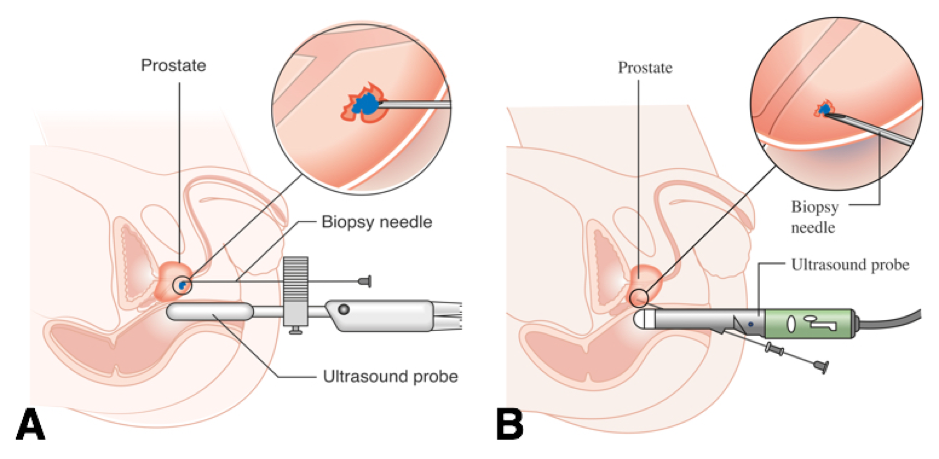
- The current standard method for diagnosing prostate cancer is through biopsies of prostatic tissue, with two potential methods:
- Rx
1.
- Acinar adenocarcinoma – originates in the glandular cells that line the prostate gland (most common)
- Ductal adenocarcinoma – originates in the cells that line the ducts of the prostate gland (~grows and metastasises faster than acinar adenocarcinoma)
- age, ethnicity: afro, FHx, BRCA2 or BRCA1 gene
- weak urinary stream, increased urinary frequency, and urgency DRE
4.
- Benign prostatic hyperplasia (BPH): a non-cancerous enlargement of the prostate gland, will also cause LUTS symptoms initially
- Prostatitis: inflammation of the prostate gland. Patients usually present with perineal pain, with neutrophils seen on urinalysis
- Other causes of haematuria: these may include bladder cancer, urinary stones, urinary tract infections and pyelonephritis
- PSA (BPH, prostatitis, vigorous exercise, ejaculation, and recent DRE, reducing its sensitivity)
free: total PSA ratio, can be used to increase the accuracy of the test for men with PSA from 4-10; a low free:total ratio is associated with an increased chance of diagnosing prostate cancer
PSA density can also be used, which is the serum PSA level divided by prostate volume determined by imaging (i.e. TRUS, CT, or MRI); higher PSA densities can suggest an increased likelihood of prostate cancer.
6.
- Transperineal (Template) biopsy (Fig. 3A) – day case under general anaesthetic, better access to the anterior part of the prostate and also has a lower risk of infection
- TransRectal UltraSound-guided (TRUS) biopsy (Fig. 3B) – this involves sampling the prostate transrectally, usually under local anaesthetic. Generally 12 cores are taken bilaterally in equal distribution from base to apex. Transrectal biopsies are associated with a 1-2% risk of sepsis.
imaging
- Multi-parametric magnetic resonance imaging
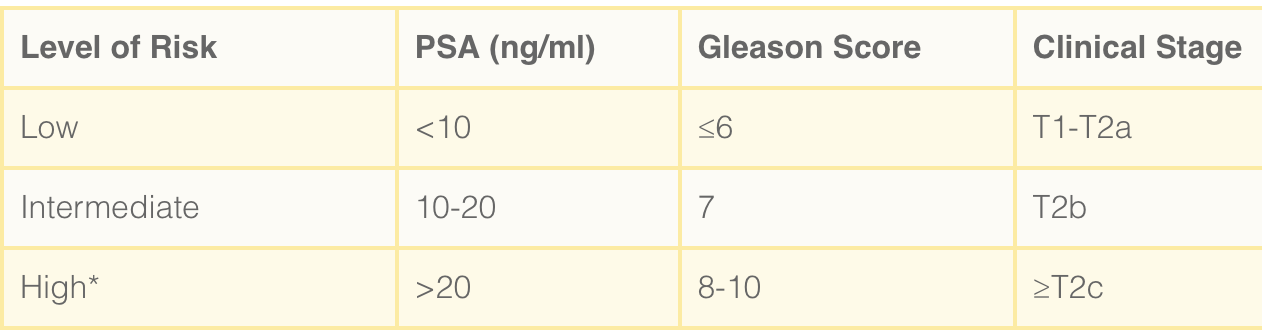
- Staging of prostate cancer is typically done for men with intermediate and high-risk disease. Staging is accomplished with abdomino-pelvic CT imaging and bone scan.
7.
- Low risk disease: active surveillance, radical treatments if disease progression
- Intermediate and high risk disease: Radical treatment, intermediate also offered active surveillance (should not be offered for high risk disease)
- Metastatic disease: Chemotherapy agents + anti-hormonal agents
- Castrate–resistant disease: evidence of hormone-relapsed disease can be considered for further chemotherapy agents, such as Docetaxel. Corticosteroids can be offered as third-line hormonal therapy after androgen deprivation therapy and anti-androgen therapy to men with hormone-relapsed prostate cancer
Active surveillance:
monitoring of patients with 3-monthly PSA, 6 month to yearly DRE, and re-biopsy at 1-3 yearly intervals assessing for progression and intervening at the appropriate time. Mp-MRI is also being used increasingly in AS protocols.
Surgery
Radical prostatectomy: removal of the prostate gland, seminal vesicles, surrounding tissue +/- dissection of the pelvic lymph nodes
open approach, laparoscopically or robotically
s/e: ED (affecting 60-90% of men), stress incontinence and bladder neck stenosis.
Radiotherapy
External-beam radiotherapy and brachytherapy are both (curative intervention* localised pr ca)
Brachytherapy: transperineal implantation of radioactive seeds (usually Iodine-125) directly into the prostate gland
External-beam radiotherapy uses focused radiotherapy to target the prostate gland and limiting damage to surrounding tissues.
Chemotherapy and Anti-Androgen Therapy (~metastatic prostate ca)
e.g.
- docetaxel (men with testosterone-resistant cancer)
- cabazitaxel (+ prednisolone, relapsed prostate cancer which has progressed after using docetaxel chemotherapy).
- cancer growth is stimulated by circulating androgens (testosterone), androgen deprivation therapies are regularly used: either LHRH agonists (e.g. goserelin or triptorelin) or GnRH receptor agonists (e.g. degarelix). Alternatively, another method of androgen deprivation is through an orchidectomy.
Newer hormone therapies: enzalutamide and abiraterone, acting to lower levels of serum testosterone (metastatic prostate cancer)
Pyelonephritis (W, 15-29, complicated/uncomplicated)
- P
most common organism*
- RF
- CF
- DD
- Ix
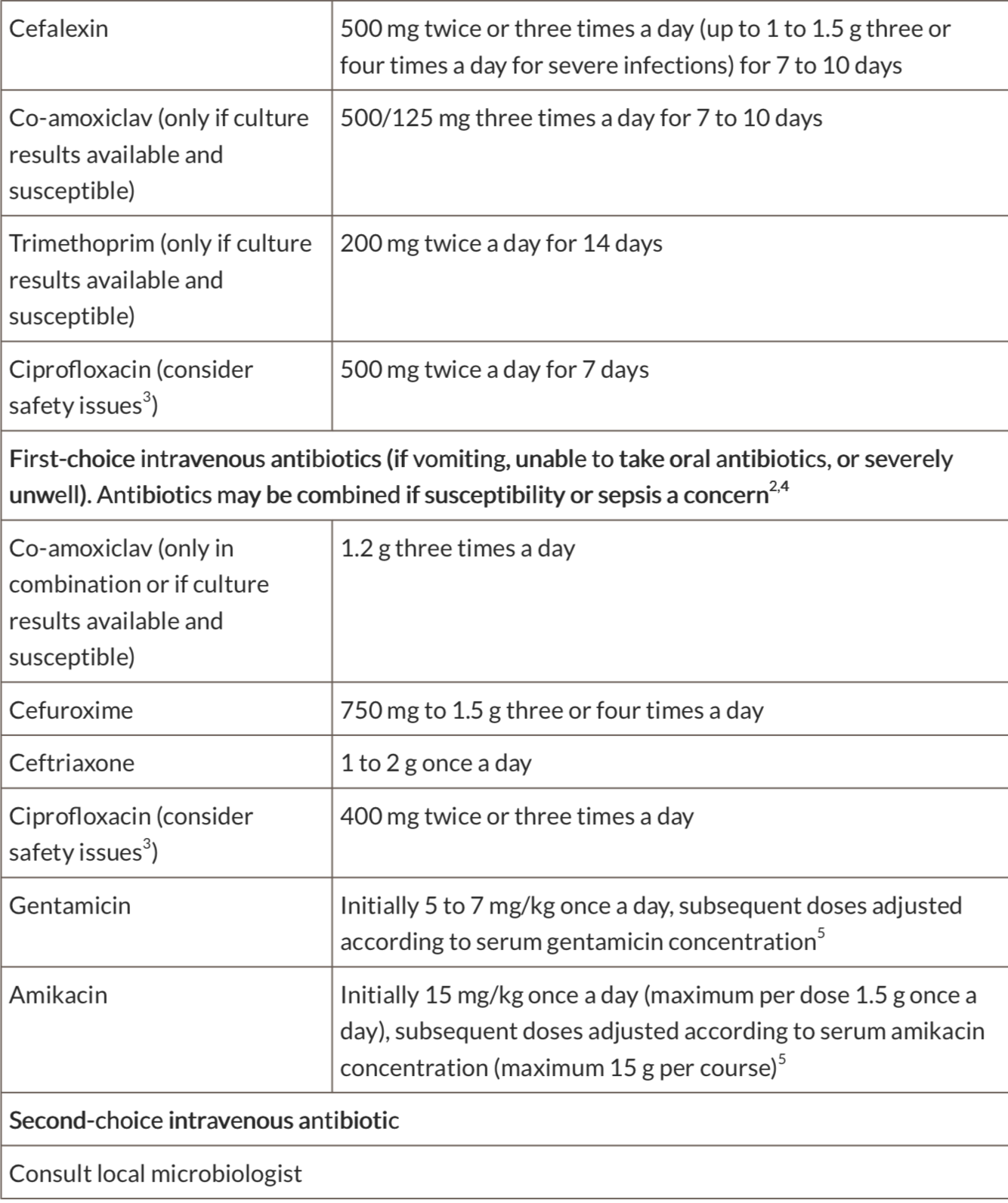
- Rx
- Complications
- ascending from the LUT, directly from the blood stream (septicaemia or IE), rarely via lymphatics (retroperitoneal abscess)
suppurative inflammation
(~80%) isolated is Escherichia coli. Others: Klebsiella, Proteus, Enterococcus faecalis (catheters), Staphylococcus aureus (catheters), Staphylococcus saprophyticus (commensal), and Pseudomonas (catheters).
*Rarely, Mycobacterium spp, yeasts, or other fungi can be the cause in immunocompromised patients
2.
Factors reducing antegrade flow of urine
- Obstructed urinary tract e.g. BPH
- Spinal cord injury - neuropathic bladder
Factors promoting retrograde ascent of bacteria
- Female gender (due to a short urethra)
- Indwelling catheter or ureteric stents / nephrostomy tubes in-situ
- Structural renal abnormalities e.g. vesico-ureteric reflux (VUR)
Factors predisposing to infection or immunocompromise
- DM, corticosteroid use, HIV infection (untreated)
Factors promoting bacterial colonisation
- Renal calculi
- Sexual intercourse
- Oestrogen depletion (menopause)
- fever, loin pain, nausea & vomiting (24-48 hours)
co-existing LUT infection (frequency, urgency, dysuria), as well as visible (or non-visible) haematuria.
costovertebral angle tenderness
Assess the patient’s fluid status and measure any post-void residual volumes.
- potential ruptured AAA, renal calculi, acute cholecystitis, ectopic pregnancy or pelvic inflammatory disease, lower lobe pneumonia, or diverticulitis
- urinalysis
beta-hCG
Routine bloods: FBC and CRP for evidence of inflammation and U&Es, to assess renal function
renal US scan
non-contrast CT imaging of the renal tract should be performed (CT KUB)
6.
- severe sepsis and multi-organ failure, renal scarring leading to CKD, pyonephrosis, and even preterm labour in pregnant women
Chronic Pyelonephritis - leading to fibrosis(scarring) and ultimately destruction of the kidney
more common in obstructed systems resulting in urinary reflux, such as strictures caused by UTIs, VUR, other anatomical abnormalities. The diagnosis if often made radiologically when evidence of a small, scarred shrunken kidney is seen
Emphysematous pyelonephritis is a rare and severe form of acute pyelonephritis, caused by gas-forming bacteria, and is associated with a high-mortality rate.
It present similar to acute pyelonephritis, however typically with fail to respond to empirical IV antibiotics. CT imaging will show evidence of gas within and around the kidney.
It is most common in diabetic patients, as the high glucose allows CO2 production from fermentation by enterobacteria.
Mild cases can be treated with broad-spectrum anti-microbial cover. Severe cases may warrant either nephrostomy insertion or percutaneous drainage of any collections present; in some cases, nephrectomy may be required
RENAL STONES iliac vessels cross the ureters -> pelvic brim
- Around 80% of urinary tract stones are made of ?
The remaining stones compositions:
- P
- CF
- Ix
- Rx
- Criteria that often warrant the need for hospital admission include:
- Complications
- Bladder Stones (chronic urinary retention, secondary to infections (classically schistosomiasis) or passed ureteric stones)
- calcium oxalate (35%), calcium phosphate (10%), or mixed oxalate and phosphate (35%)
struvite stones* (magnesium ammonium phosphate), urate stones (the only radiolucent stones), and cystine stones (typically associated with familial disorders affecting cystine metabolism).
*Struvite stones are often large soft stones, most common cause of “staghorn calculi”
- urate stones: high levels of purine in the blood, either from diet (e.g. red meats) or through haematological disorders (such as myeloproliferative disease), results in increase of urate formation from the purine breakdown, leading to crystalisation in the urine.
cystine stones: hypocystinuria, an inherited defect that affects the absorption and transport of cystine in the bowel and kidneys. As citrate is a stone inhibitor, hypocitraturia from the condition can predispose to stone formation
- sudden onset, flank to pelvis
- urinalysis, bloods, Urate and calcium levels, stone analysis, non-contrast CT scan, Ultrasound scans, hydronephrosis
- Initial
- fluid resuscitation (vomitting)
- ~conservative: lower ureter or <5mm in diameter
- analgesia (opiate, NSAIDs per rectum)
- sepsis -> IV antibiotic therapy and urgent referral to the urology team
Stent Insertion or Nephrostomy
neither options are definitive, however can temporarily relieve symptoms prior to definitive management.
- Retrograde stent insertion: stent within the ureter, approaching from distal to proximal via cystoscopy. It allows the ureter to be kept patent and temporarily relieve the obstruction.
- Nephrostomy is a tube placed directly into the renal pelvis and collecting system, relieving the obstruction proximally. If required, an anterograde stent can subsequently be passed via the same tract made.
Definitive Management
- Extracorporeal Shock Wave Lithotripsy (ESWL): targeted sonic waves to break up the stone, to then be passes spontaneously. This is typically reserved for small stones (<2cm), performed via radiological guidance (either X-ray or ultrasound imaging). CI: pregnancy or stone positioned over a bony landmark (e.g. pelvis)
- Percutaneous nephrolithotomy (PCNL): renal stones only, being the preferred method for large renal stones (including staghorn calculi). Percutaneous access to the kidney is performed, with a nephroscope passed into the renal pelvis. The stones can then be fragmented using various forms of lithotripsy.
- Flexible uretero-renoscopy (URS): passing a scope retrograde up into the ureter, allowing stones to be fragmented through laser lithotripsy and the fragments removed.
6.
- Post-obstructive AKI
- Uncontrollable pain from simple analgesics
- Evidence of infected
- Large stones (>5mm)
7.
infection and post-renal acute kidney injury
Recurrent renal stones can lead to renal scarring and loss of kidney function
- LUTs symptoms and require investigation the same as for renal and ureteric stones.
Definitive management is through cystoscopy, allowing the stones to drain or fragmenting them through lithotripsy if required.
Bladder stones often occur, especially if the underlying cause is not addressed. The chronic irritation of the bladder epithelium can also predispose to the development of TCC bladder cancer.
BENIGN PROSTATIC HYPERPLASIA
- prostate function
- RF
- CF
- what is the IPSS
- DD
- Ix
- Rx
- Complications
- testosterone to dihydrotestosterone (DHT) using the enzyme 5α-reductase
- age, afro, FHx
- voiding symptoms (hesitancy, weak stream, terminal dribbling, or incomplete empyting) or storage symptoms (urinary frequency, nocturia, nocturnal enuresis, or urge incontinence)
DRE firm, smooth, symmetrical prostate
- image
5.
- Prostate cancer: patients may present with LUTS, however an asymmetrical craggy/nodular prostate and raised PSA are indicative of prostate cancer
- UTI: the addition of dysuria, loin or suprapubic pain, or pyrexia, in the presence of a nitrite- and/or leucocyte-positive urine dip
- Overactive bladder: although the patient will present with LUTS, bladder ultrasound will show a low post-void residual volume.
- Bladder cancer: haematuria is likely to be the predominant
- urinary frequency and volume chart
urinalysis
post-void bladder scan
Prostate Specific Antigen (PSA)
ultrasound scan
Urodynamic studies can give objective measurements related to reported symptoms, including bladder contractility, flow rate, and storage capacity. The bladder outlet obstruction index (BOOI) can help diagnose obstructive voiding related to BPH*
- symptom diary, providing a medication review (especially iatrogenic causes of LUTS), and giving suitable lifestyle advice (e.g. moderating caffeine and alcohol intake) are helpful conservative options that can be done for all patient
Medical
- α-adrenoreceptor antagonist (α-blockers) e.g. tamsulosin (relax prostatic smooth muscle)
postural hypotension, asthenia, rhinitis, retrograde ejaculation, and Floppy Iris Syndrome (occurs intra-operatively in those undergoing cataract surgery)
- 5α-reductase inhibitors e.g. Finasteride
prevent the conversion of testosterone to DHT, resulting in a decrease in prostatic volume
Surgical
- TransUrethral Resection of the Prostate (TURP)
endoscopic removal of obstructive prostate tissue using a diathermy loop to increase the urethral lumen size
Complications: haemorrhage, sexual dysfunction, retrograde ejaculation, and urethral stricture
- A Holmium Laser Enucleation of the Prostate (HoLEP)
Holmium:YAG laser used to heat and dissect sections of prostate into the bladder. It is becoming increasing more prevalent in use due to excellent outcomes and reduced post-operative complications, its use only being limited due to it being a technically challenging procedure.
- PVP (Photoselective Vaporization of the Prostate)
- TUVP (Transurethral Vapourization of the Prostate)
- TUMT (Transurethral Microwave Thermotherapy).
- Although used less commonly simple prostatectomy using open or minimally invasive surgical techniques remain an option for patients with large prostates
8.
- High-pressure retention, where chronic or acute-on-chronic urinary retention results in a post-renal kidney injury. Other complications of the condition include recurrent UTIs or significant haematuria episodes.
- TURP Syndrome
TURP using monopolar energy requires use of hypoosmolar irrigation during the procedure which can result in significant fluid overload and hyponatremia as the fluid enters the circulation through the exposed venous beds.
Patients with TURP syndrome present with confusion, nausea, agitation, or visual changes and needs urgent management by addressing the fluid overload and carefully reducing the level of hyponatremia. Fortunately, TURP syndrome is increasingly rare due to the use of bipolar energy which uses isotonic irrigation fluids.
PROSTATITIS (acute bacterial prostatitis, chronic bacterial prostatitis, nonbacterial prostatitis, and prostatodynia)
- P
- RF
- CF
- Investigations
- Rx
- E. Coli (most common), Enterobacter, Serratia, Pseudomonas, and Proteus species. Sexually transmitted infections, such as Chlamydia or Gonorrhoea, are a rare cause.
- For acute bacterial prostatitis:
- Indwelling catheters
- Phimosis or urethral stricture
- Recent surgery, including cystoscopy or transrectal prostate biopsy
- Immunocompromised
In addition, for chronic prostatitis:
- Intraprostatic ductal reflux
- Neuroendocrine dysfunction
- Dysfunctional bladder
- LUTS, features of systemic infection (including pyrexia), perineal or suprapubic pain, or urethral discharge
tender and boggy prostate
Chronic prostatitis should be suspected in men who complain of pelvic pain or discomfort >3 months (Prostatodynia), alongside LUTS; the perineum is the most common site for pain, however pain can occur in the suprapubic region, lower back, or rectum
- Urine culture are the first line investigations*
STI screen and routine bloods, including FBC, CRP, and U&Es (prostate specific antigen (PSA) will often be elevated in cases, therefore is not routinely performed).
pts failed to respond to antibiotic therapy, other pathologies such as prostate abscess need to be ruled out using transrectal prostatic ultrasound (TRUS) or CT imaging.
*Meares and Stamey’s 4 cups urinary sediment were previously used, but due to poor practicality and time consumption, they are now rarely used in current practice.
5.
- prolonged abx e.g. quinolone (good penetration into the prostate)
- suitable analgesia (~paracetamol and NSAIDs)
- Alpha blockers or 5a-redictase inhibitors (2nd line) esp for chronic prostatitis cases.
- severely ill admission to hospital may be necessary. Specialist input may be required those patients with diabetes mellitus, long-term catheter, immunocompromised, or suspected prostatic abscess.
- Those with pre-existing urological condition (e.g. BPH) may warrant referral to urology following the treatment of the acute infection for further management.
Further Management
- Significant LUTS can be managed well with a 4-6-week trial of an alpha blocker (e.g. doxazosin, terazosin, tamsulosin). A 6-week course of antibiotics may also be warranted if symptoms have been present for less than 6 months.
- chronic pain specialist. For CPPS, psychological therapies are an additional therapeutic option. An MDT approach (urologists, pain specialists, specialist physiotherapists, GPs, cognitive behavioural therapists, sexual health specialists) is recommended for optimal outcome.
EPIDIDYMITIS
- P
- RF
- CF
- DD
- Ix
- Rx
- M <35 years old, the most likely mechanism is sexual transmission, most common organisms* are N. gonorrhoeae and C. trachomatis.
*In males who practice anal intercourse, enteric organisms such as E. coli are also a common cause
In males aged >35 years old, an enteric organism from a urinary tract infection is the more likely mechanism of the disease**. Therefore, the most common pathogens are E. coli, Proteus spp., Klebsiella pneumoniae, and Pseudomonas aeruginosa.
2.
- males who have sex with males (MSM), multiple sexual partners, or a known contact of gonorrhea
- recent instrumentation or catheterisation, bladder outlet obstruction (e.g. prostate enlargement, urethral stricture), or an immunocompromised state.
3.
- unilateral scrotal pain + swelling
- Fever and rigors
- Associated symptoms (secondary to the underlying cause) may also be present, such as dysuria, storage LUTS, or urethral discharge. Ensure to clarify a sexual history in all cases.
- o/e: red and swollen
- epididymis +/- the testis will be very tender on palpation
- ?associated hydrocele
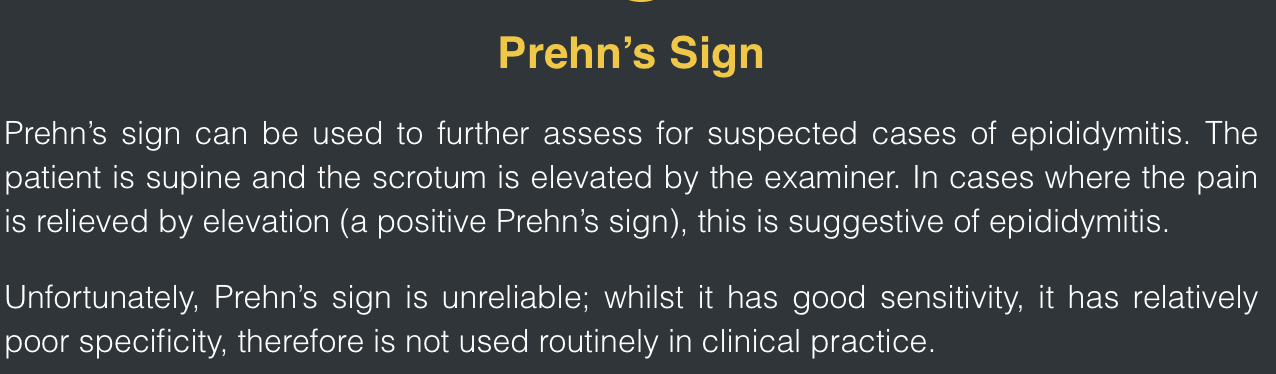
- Specific tests include assessing for the cremasteric reflex, which is intact in cases of epididymitis, and Prehn’s sign, which when positive is also suggestive of epididymitis.
- **This is often secondary to a bladder outflow obstruction from prostatic enlargement, leading to retrograde ascent of the pathogen
4.
- Testicular torsion is the most important differential, as it is a surgical emergency. Pain is more sudden onset and severe, in the absence of LUTS. Whilst US Doppler can aid in the diagnosis, any significant suspicion of torsion should warrant urgent scrotal exploration.
- testicular trauma, testicular abscess, epididymal cyst, hydrocoele, or testicular tumour
5.
- urine dipstick performed (checking for evidence of infection), with a low-threshold for sending for urine culture (MC&S)
- first-void urine should be collected and sent for Nucleic Acid Amplification Test (NAAT), to assess for N. gonorrhoeae, C. trachomatis, and M. genitalium. Further STI screening may be warranted, dependent on the history.
- Routine bloods, including FBC and CRP, can aid in the assessment for an infective cause.
Imaging
- The diagnosis of epididymitis is typically a clinical one, however ultrasound imaging of the testes via an US Doppler can be useful to confirm the diagnosis (Fig. 2)* and to rule out any complication (e.g. testicular abscess).
*A colour Doppler ultrasound scan will be able to show increased vascularity of the epididymis in suspected cases; whilst it can also be used to assess testicular blood flow, if there is suspicion of testicular torsion, the patient should be sent for scrotal exploration.
6.
Initial management
- antibiotic therapy
- analgesia
- Bed rest and scrotal support will also help in symptomatic improvement.
Current EAU Guidelines suggest first line treatments* of:
- Enteric organisms – Ofloxacin 200mg PO BD for 14 days or levofloxacin 500mg BD for 10 days
- STI organisms – Ceftriaxone 500mg IM single dose and Doxycycline 100mg PO twice daily for 10-14 days (with Azithromycin 1g PO single dose added if gonorrhoea likely)
- Patients should abstain from sexual activity until the antibiotic course is completed and symptoms resolve.
- Patients should also be counselled on appropriate barrier contraception use to reduce risk of STIs
Complications
Typically, symptoms improve within 48hrs of starting antibiotics. Complications of epididymitis can include reactive hydrocele formation, abscess formation (rare), or testicular infarction (rare).
TESTICULAR TORSION (horizontal lie to their testes, often termed a ‘bell-clapper deformity)
4-6hrs window
- RF
- CF
- DD
- Ix
- Rx
- Complications
1.
- Age (most common 12-25yrs)
- Previous testicular torsion*
- Family history of testicular torsion
- Undescended testes
2.
- sudden onset severe unilateral testicular pain
- nausea and vomiting, secondary to the pain
- Referred abdominal pain can also occur
O/e, the testis will have a high position* (compared the contralateral side) with a horizontal lie. It can also appear swollen and will be extremely tender.
cremasteric reflex is absent
pain continues despite elevation of the testicle, termed a negative Prehn’s sign (in epididymo-orchitis, Prehn’s test is often positive but this is an unreliable examination finding).
*It is often worth clarifying with the patient the normal position of their testes in their scrotum (i.e. which testis normally sits higher)
- epididymo-orchitis; this is normally associated with a more gradual onset of pain and can be associated with LUTS and / or pyrexia.
Other differentials to consider include trauma, incarcerated inguinal hernia, malignancy, renal colic, hydrocele, idiopathic scrotal oedema, and torsion of the hydatid of Morgagni.
4.
- The diagnosis of testicular torsion is a clinical one, therefore any suspected cases should be taken straight to theatre for scrotal exploration.
- However, in cases with sufficient equipoise, Doppler ultrasound can be used to investigate potential compromised blood flow to the testis (if available, this test has a high sensitivity (89%) and specificity (99%)).
- A urine dipstick can also be performed to assess for any potential infective component, as part of potential differentials.
5.
- analgesia
- anti-emetics pre-operatively
- nil by mouth
- maintenance fluids
the 6 fs before surgery
feel = analgesia food =NBM fluids= maintenance frow up= anti-emetics fibrinolysis= LMWH feel protected= prophylaxis abx
Surgical
- If torsion is confirmed intra-operatively, the cord and testis will be untwisted and both testicles fixed to the scrotum, termed bilateral orchidopexy (prevent further any further torsion episodes).
- testis is non-viable, an orchidectomy; prosthesis can be inserted at time of surgery or at a later date
- Despite expedient scrotal exploration, de-torsion, and orchidopexy, the affected testis may later undergo atrophy. Patients undergoing scrotal exploration should be consented for chronic pain, palpable suture, risk to future fertility, and a theoretical risk of future torsion despite fixation.
*Testicular salvage rates are 90-100% if surgery performed within 6hrs of onset of pain, and this decreases to 50% if symptoms are present for more than 12 hours
TESTICULAR CANCER
- classification
- RF
- dd
- Ix
- Rx
- Primary testicular tumours are categorised into:
germ cell tumours (GCT) (95%)
- Seminomas ~ benign, Leydig cell tumors or Sertoli cell tumors*
- NSGCTs: yolk sac tumors, choriocarcinoma, embryonal carcinoma, and teratoma; NSGCTs often metastasise early and have worse prognosis than seminomas.
non-germ cell tumours (NGCTs) (5%);
GCTs can be further sub-classified into seminomas and non-seminomatous GCTs (NSGCT), and are usually malignant.
2.
Cryptorchidism (undescended testes) is associated with a 4-10x higher risk of GCTs
previous testicular malignancy, a positive family history, and Kleinfelter’s syndrome.
3.
unilateral painless testicular lump.
O/e: the mass is typically irregular, firm, fixed, and does not transilluminate.
Evidence of metastasis may present with weight loss, back pain (from retroperitoneal metastases), or dyspnoea (secondary to lung metastases).
*Lymphatic drainage of the testes is to the para-aortic nodes, therefore localised lymphadenopathy may not be present, even in cases of metastatic disease
- epididymal cyst, haematoma, epididymitis, or hydrocoele
4.
- ßHCG is elevated in 60% of NSGCTs and 15% of seminomas
- AFP can be raised in some NSGCTs as well
- LDH can also be used as a surrogate marker for tumour volume.
*Levels can be used post-treatment to determine its efficacy
Scrotal ultrasound should be used in the initial assessment of scrotal lumps, alongside concurrent tumour markers. The disease will then be staged via CT imaging with contrast of the chest-abdomen-pelvis.
Crucially, a trans-scrotal percutaneous biopsy should not be performed, as it might cause seeding of the cancer. Diagnosis is made through tumour marker and imaging alone.
5.
- Most cases suitable for surgery will undergo an inguinal radical orchidectomy (removes the testes along with the spermatic cord, allowing for maximal lymphatic system to be removed)
- Sperm abnormalities and Leydig cell dysfunction are frequently found in patients with testicular cancer prior to orchiectomy. Furthermore, chemotherapy and radiation treatment can additionally impair fertility. Therefore, in patients in the reproductive age group, pre-treatment fertility assessment should be performed, and semen analysis and cryopreservation offered accordingly
Non-Seminomatous Germ Cell Tumours
Stage 1 NSGCTs will require orchidectomy then further managed dependent on their risk score. Low risk patients without any evidence of vascular invasion can routinely enter just surveillance, whilst high risk patients or those with vascular invasion require adjuvantchemotherapy (typically cisplatin, etoposide, bleomycin) and then surveillance
Metastatic NSGCTs management is also dependent on risk scoring. Cases with intermediate prognosis should be treated with cycles of chemotherapy, whilst those with poor prognosis should be treated with one cycle of chemotherapy before reassessment(those with marker decline should have continued chemotherapy cycles, whilst those with unfavourable decline should have their chemotherapy intensified).
Seminomas
Stage 1 seminoma can often be managed with orchidectomy alone and surveillance monitoring. Patients have a high relapse risk are often considered for chemotherapy.
For metastatic seminoma, stage IIA can be treated with either radiotherapy orchemotherapy, whilst higher stage disease will require primary chemotherapy and treated similar to metastatic NSGCTs (as above).
URETHRITIS (gonococcal urethritis and non-gonococcal urethritis)
- RF
- cf
- DD
- Ix
- <25yrs, men who have sex with men, previous STI, recent new sexual partner, or more than one partner in the last year.
- dysuria, penile irritation, and discharge
reiters: oligoarthritis, lower joints, conjunctivitis, Keratoderma blennorrhagicum
3.
Balanitis, inflammation of the glans penis, presents with pruritis, erythema and discharge between the foreskin and the glans, contrasting with the urethral discharge and dysuria of urethritis. common in older patients and can be secondary to bacterial or fungal infection.
Acute prostatitis may present with LUTS, ejaculatory pain, and pain in the penis, perineum, or rectum. Any urethral discharge present is often blood-tinged.
Cystitis presents with dysuria and frequency, however rarely is associated with urethral discharge.
- urethral swabs
-
Orthopaedics - Clinical conditions49
-
Drugs57
-
Pain management1
-
DVT assessment & management15
-
Care of the diabetic surgical patient and the surgical patient on steroids.38
-
peri operative42
-
peri op (general)18
-
Period Cardioresp8
-
General surgery43
-
GP day cases55
-
Medicine day case23
-
Hepato pancreatic biliary surgery7
-
contraception10
-
Rheumatology56
-
Paediatrics35
-
geri27
-
Urology10
-
Vascular surgery17
-
ID19
-
Renal workbook21
-
surgery workbook16
