KIDNEY ANATOMY
Does US over or under estimate renal length?
Ultrasound (US) often underestimates the true renal length because of technical difficulties in imaging the entire kidney.
19F Hypertensive
kypokalaemia
elevated aldosterone
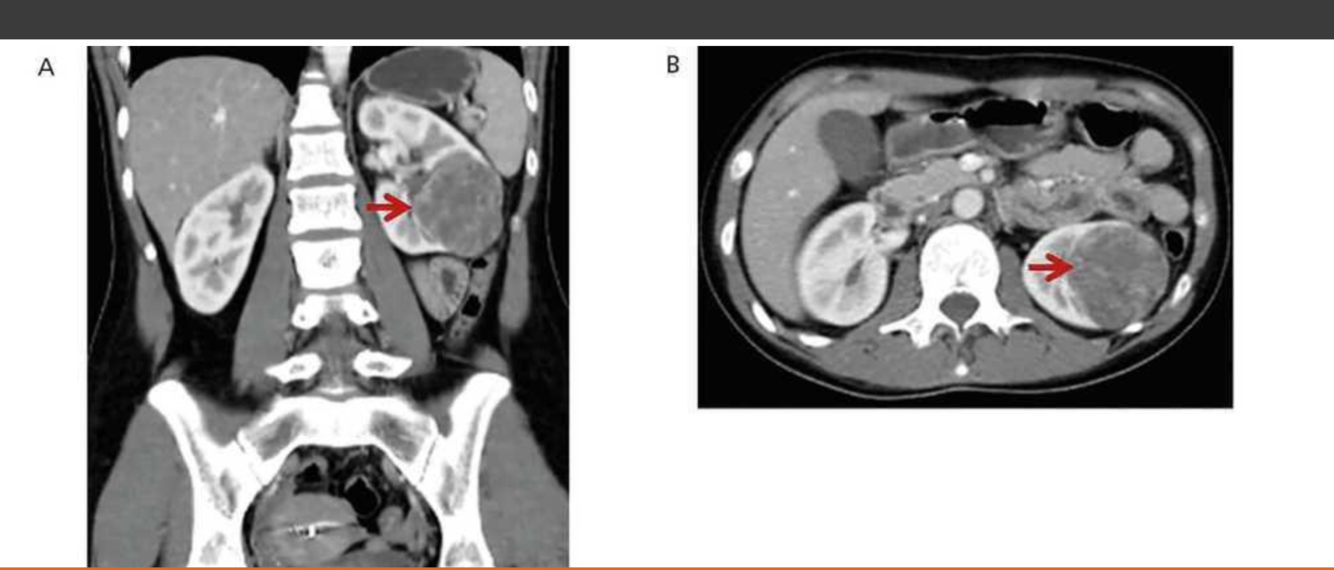
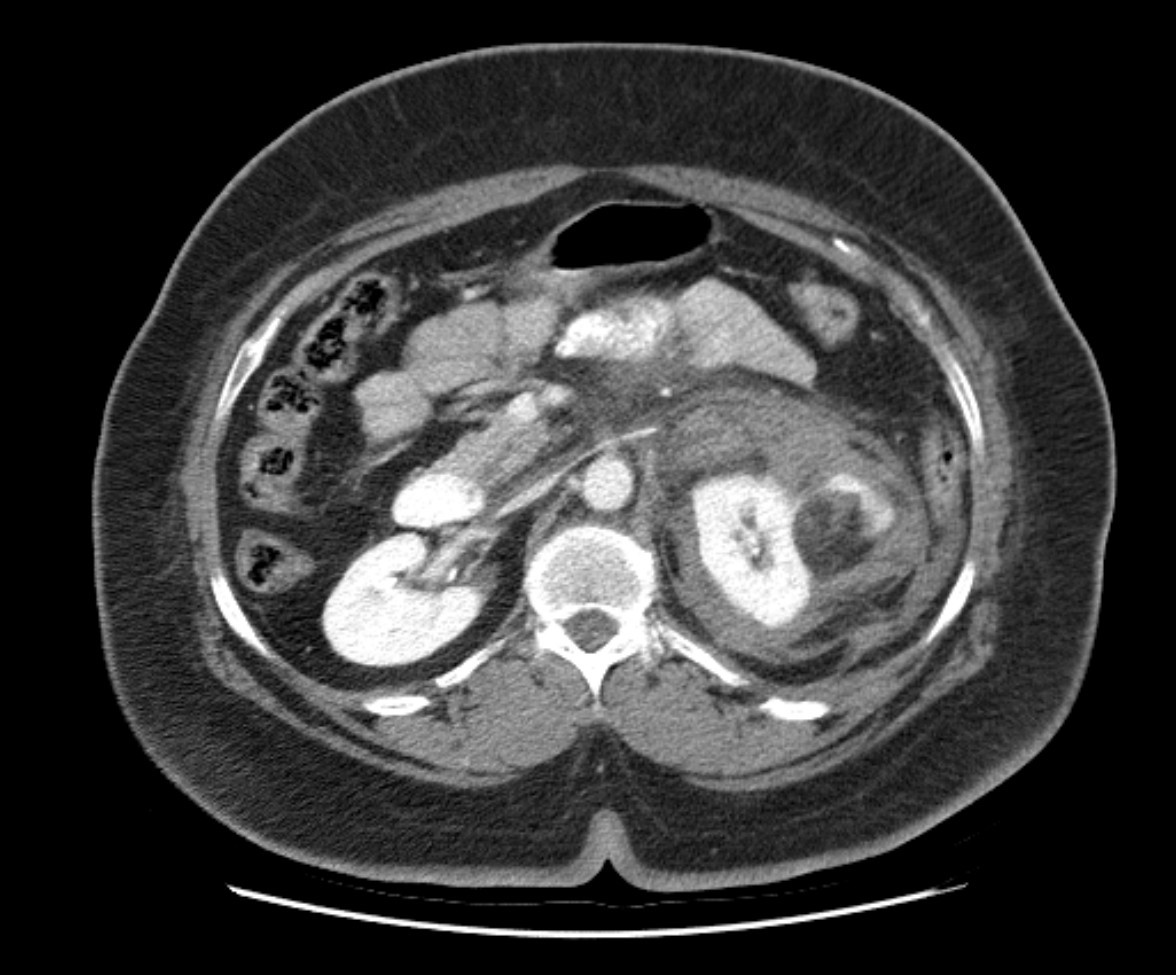
Juxtaglomerular Tumor (Reninoma)
- Secretion of renin causes HTN, hypernatremia, and hypokalemia (secondary aldosteronism).
- Most patients undergo angiography as part of the workup for HTN.
- Tumors appear as small hypovascular masses. Rare.
Reninoma is a tumour of the cells of the juxtaglomerular apparatus that produces excessive amounts of renin, resulting in a secondary form of hyperaldosteronism, manifesting clinically with hypertension (HT) and hypokalaemia1. This renal tumour is predominant in females, with a peak incidence between the second and third decade of life and, although uncommon, it is a treatable cause of HT2. It should be suspected in any patient with refractory HT associated with hypokalaemia and high levels of aldosterone.
We present the first case of reninoma reported in Argentina in a young woman with refractory HT and hypokalaemia.
In 1967, Robertson et al.6 reported the first renin-producing tumour. Kihara et al. later called them “juxtaglomerular cell tumours”7. These tumours are very uncommon, with their incidence peaking between the second and third decade of life and they are predominantly found in females, originating in the myoendocrine cells of the renal juxtaglomerular apparatus, although the production of renin by different tumours has also been demonstrated, such as Wilms tumours, carcinoid tumours, renal oncocytoma and renal cell carcinoma8,9. In accordance with the presence or absence of symptoms, JCT may occur as: a “typical” variant in the majority of cases and manifests with HT, hypokalaemia, high plasma renin and secondary hyperaldosteronism; an “atypical” variant, in which HT is not accompanied by hypokalaemia; and a third “non-functioning” variant, which occurs without HT and with normal levels of potassium10,11.
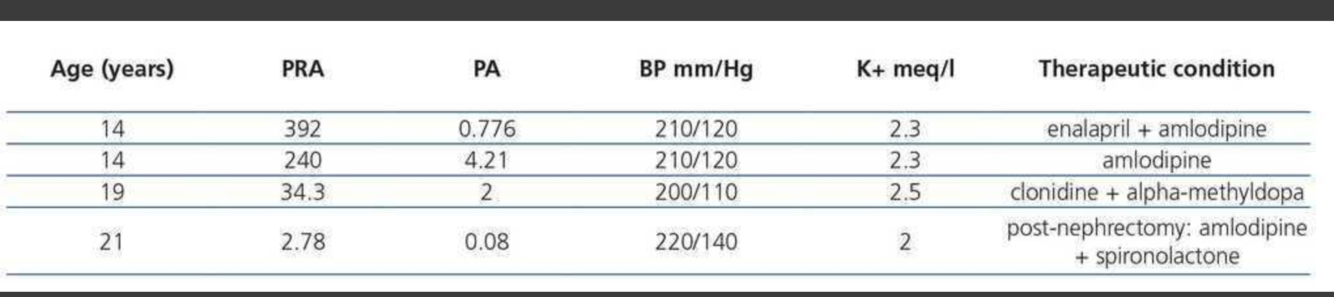
Plasma renin activity (PRA) and plasma aldosterone (PA)
https://www.revistanefrologia.com/en-juxtaglomerular-cell-tumour-as-curable-articulo-X2013251415054971
SIGN
What sign is this and what does it indicate?

Case Discussion
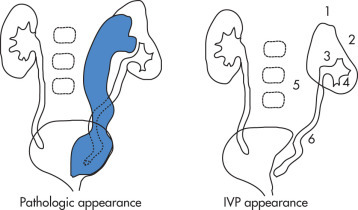
Left sided duplicated collecting system with the upper moiety obstruction, and non-functioning. It displaces the lower pole moiety inferiorly, mimicking the appearance of a drooping lily.
The drooping lily sign refers to the inferolateral displacement of the opacified lower pole moiety due to an obstructed (and unopacified) upper pole moiety in duplicated collecting system.
Case courtesy of Dr Mohammad Taghi Niknejad, Radiopaedia.org, rID: 54354
What are the 6 radiographic features of uretal duplication?
What sign is this?

Radiographic Features (Lebowitz) ( Fig. 11.39 )
- Increased distance from top of nephrogram to collecting system: hydronephrotic upper pole moiety causes mass effect (1)
- Abnormal axis of collecting system (2)
- Concave upper border of renal pelvis (3)
- Diminished number of calyces compared with normal side; drooping lily sign (4)
- Lateral displacement of kidney and ureter (5)
- Spiral course of ureter (6)
- Filling defect in the bladder (ureterocele)
Case courtesy of Dr Mohammad Taghi Niknejad, Radiopaedia.org, rID: 54354
What is a renal Adenoma?
Adenoma
Best described as adenocarcinoma with no metastatic potential. Usually detected at autopsy.

Peripelvic Cyst
- Originates from sinus structures, most likely lymphatic in origin
- May be indistinguishable from hydronephrosis on US, requiring an IVP or CT for definitive diagnosis
- Attenuated, stretched infundibula
- IVP differential diagnosis (DDx): renal sinus lipomatosis

PATHOLOGICAL SPECIMEN
- What is the inheritance pattern?
- What is the incidence?
- What are the clinical findings?
- What is the treatment?
- What is the malignancy risk?
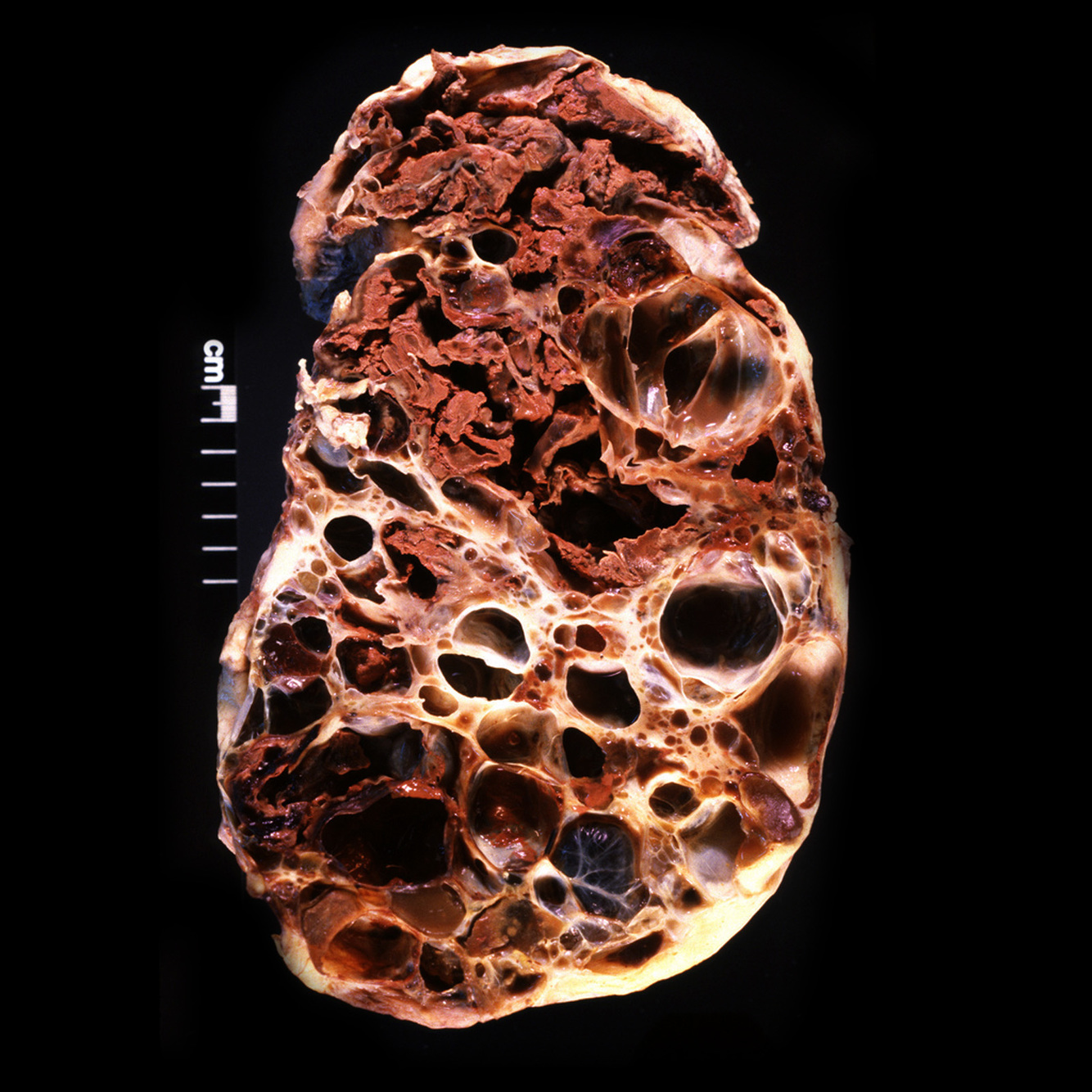
Adult Polycystic Kidney Disease (Apkd) ( Fig. 4.5 )
- Intro:
- Cystic dilatation of collecting tubules, as well as nephrons
- (unlike MCD and infantile polycystic kidney disease in which only the collecting tubules are involved).
- AD trait (childhood type is AR).
- Incidence:
- 0.1% (most common form of cystic kidney disease; accounts for 10% of patients on chronic dialysis).
- Clinical
- Slowly progressive renal failure.
- Symptoms usually begin in 3rd or 4th decade, but clinical onset is extremely variable, ranging from palpable cystic kidneys at birth to multiple cysts without symptoms in old age.
- Enlarged kidneys may be palpable.
- Treatment
- Treatment is with dialysis and transplant.
- Malignancy
- No increased risk of malignancy.

What are the complications of RF Ablation (re RCC)?
Complications
- Pain may last for several days to weeks.
- Postablation syndrome:
- fever, malaise, and body aches.
- Severity is related to volume of tissue ablated.
- Hemorrhage, often self-limited
- Injury to ureter, central collecting system, or adjacent organs
What are the 6 associations of this condition?

Horseshoe Kidney
- Associations
- UPJ obstruction, 30%
- Ureteral duplication, 10%
- Genital anomalies
- Other anomalies: anorectal, cardiovascular, musculoskeletal anomalies
Case courtesy of Dr Aditya Shetty, Radiopaedia.org. From the case rID: 27958
What is the staging for this condition?

Renal pelvis TCC
Staging
- Stage I: mucosal lamina propria involved
- Stage II: into, but not beyond, muscular layer
- Stage III: invasion of adjacent fat/renal parenchyma
- Stage IV: metastases
Medullary Cystic Disease
What is the cause of this disease?
Medullary Cystic Disease (MCD) ( Fig. 4.4 )
Spectrum of diseases characterized by tubulointerstitial fibrosis.
Patients usually present with azotemia and anemia and subsequently progress to end-stage failure.
Azotemia: Elevated levels of urea and other nitrogen compounds in the blood.
SYNDROMES
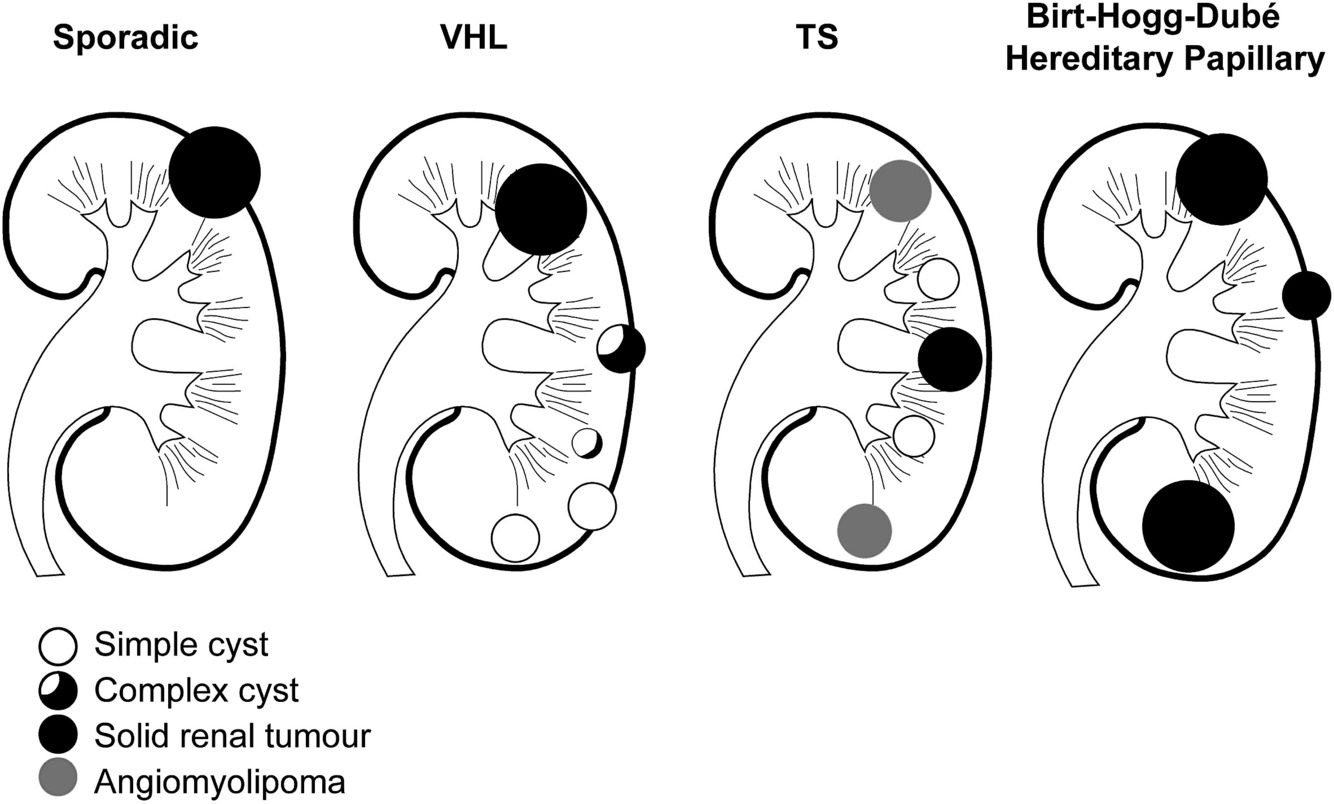
What syndromes/diseases are a/w renal Cysts?
What are the differences in the morphology of the cysts?
- TS
- VHL
- BHD
- ARPCKD
- ADRCKD
- DICER
- Nephronopthisis
- Asphyxiating thoracic dys- trophy (Jeune syndrome)
- Meckel-Gruber syndrome;
- Joubert syndrome and related disorders;
- Ellis–van Creveld syndrome;
- short rib–polydactyly group
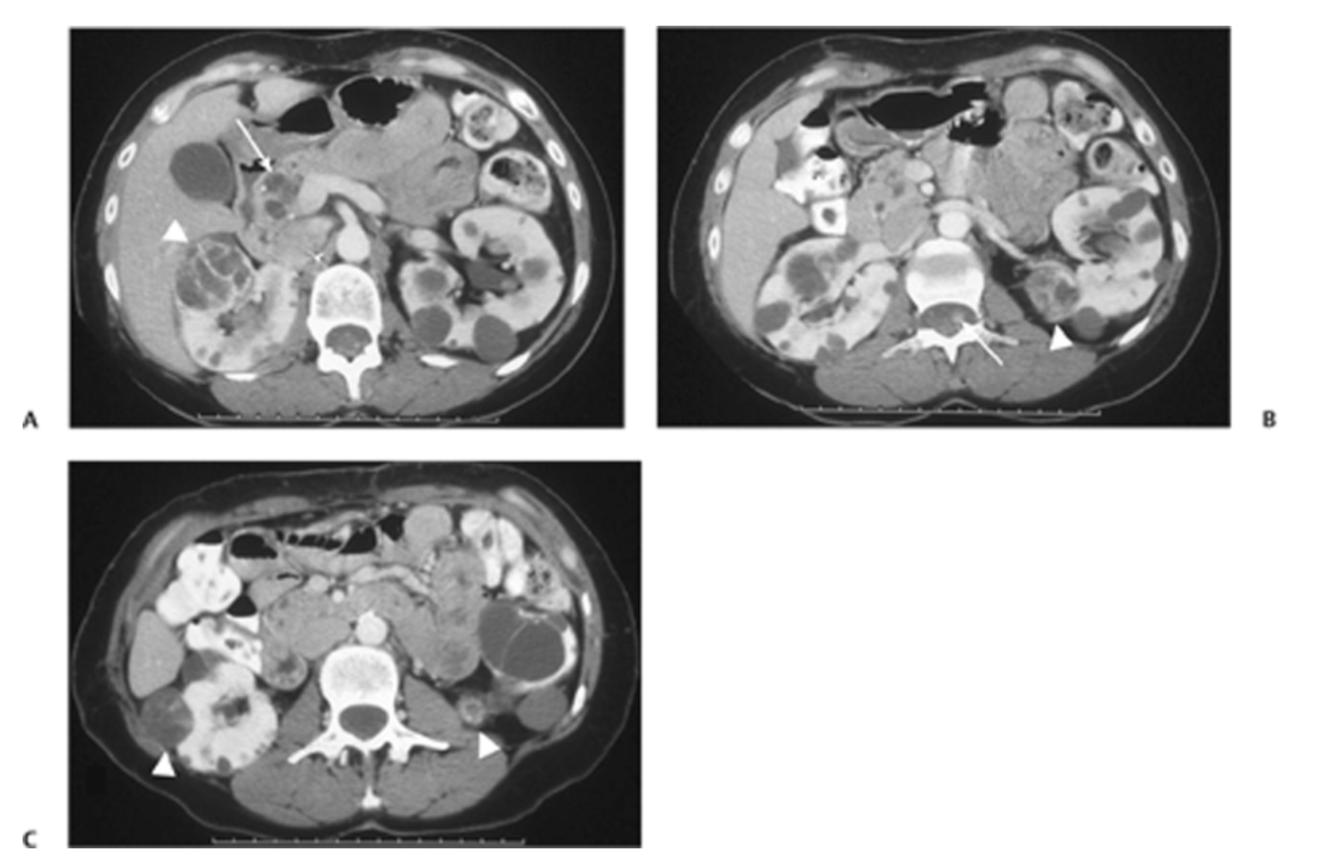
Fig. 63.1 (A) Postcontrast CT image shows bilateral renal cysts. There is a large cyst within the right kidney with thick enhancing septations (arrowhead). Note the multiple pancreatic cysts (arrow). (B) Axial image shows a mixed solid and cystic lesion in the left kidney (arrowhead), along with an enhancing nodule in the chord (arrow). (C)An additional complex cyst with enhancing septation is seen in the right kidney (arrowhead), along with a small enhancing lesion in the left kidney (arrowhead).
SYNDROMES
Re ADPCKD describe the following:
Type of inheritance?
Genes?
Renal findings?
Associated findings?
AD
PKD1, PKD2
(ciliopathy)
Multiple bilateral variably sized renal cortical and medul-
lary cysts; number and size
of cysts increase with time; nephrolithiasis; chronic kidney disease typically occurs in late adulthood
Ductal plate malformations (eg, congenital hepatic fibrosis); extrarenal cysts (eg, liver, pancreas, seminal vesicles); intracranial aneu- rysms (typically in adult- hood)
Describe the staging system of RCC
Staging
- Stage I:
- tumor confined to kidney
- Stage II:
- extrarenal (may involve adrenal gland) but confined to Gerota fascia
- Stage III:
- A: venous invasion (renal vein);
- B: lymph node metastases;
- C: both
- Stage IV:
- A: direct extension into adjacent organs through Gerota fascia;
- B: metastases
- Lungs, 55%
- Liver, 25%
- Bone, 20% (classic lesions are lytic, expansile)
- Adrenal, 20%
- Contralateral kidney, 10%
- Other organs, <5%

Complicated Cysts
- Complicated cysts are cysts that do not meet the criteria of simple cysts and thus require further workup.
- Case Discussion
- This is a classic example of a Bosniak type IV cyst - with an abnormal cyst first identified on ultrasound proceeding to three phase CT imaging.
- It is made more difficult by the bilateral cystic renal disease, but the left mid/upper pole cyst contained a significant solid element.
- The patient is due for a total nephrectomy - the histopathological outcome will be added when available.
Case courtesy of Dr Ian Bickle, Radiopaedia.org, rID: 24244
KIDNEY ANATOMY
L and R kidneys should be within x cm of eachother?
Left and right kidney size should not vary more than 1cm.
What is the prognosis of RCC?
5 yr survival
Stage 1, 2, 3, 4?
What are the unual behaviours of RCC?
Prognosis
5-year survival:
- stage I = 81%
- stage II = 74%
- stage III = 53%
- stage IV = 8%
- Tumors often have atypical behavior:
- Late recurrence of metastases:
- 10% recur 10 years after nephrectomy.
- Some patients survive for years with untreated tumor.
- Spontaneous regression of tumor has been reported but is very rare.
- Late recurrence of metastases:

Dromedary hump: parenchymal prominence in left kidney; results from compression of adjacent spleen
Case courtesy of Assoc Prof Craig Hacking, Radiopaedia.org, rID: 53697
Angiomyolipoma (Aml)
- Hamartomas containing fat, smooth muscle, and blood vessels.
- Small lesions are not treated; large and symptomatic lesions are resected or embolized.
- Unlikely to bleed if <4 cm.
- Complication: tumors may spontaneously bleed because of their vascular elements.
Case courtesy of Dr Behrang Amini, Radiopaedia.org, rID: 35925
Axial CT through the kidneys shows a fat-attenuation lesion in the left kidney with a perirenal collection, most likely blood. This is consistent with a bleeding angiomyolipoma.
What are the 4 types of this condition?
Medullary cystic disease
Types
- Familial nephronophthisis, 70%, autosomal recessive (AR)
- Juvenile type, onset at age 3–5 years (most common)
- Adult MCD, 15%, autosomal dominant (AD)
- Renal-retinal dysplasia, 15%; recessive associated with retinitis pigmentosa
Radiopedia
- Medullary cystic disease complex belongs to group of paediatric cystic renal diseases characterised by progressive tubular atrophy with glomerulosclerosis (chronic tubulointerstitial nephritis) and multiple small medullary cysts.
- Epidemiology
- There is no recognised gender predilection
- Clinical presentation
- Presentation with polydipsia and polyuria, due to initial tubular injury, tends to progress to end stage renal failure, growth retardation, lethargy.
- Three clinical variants based on age of onset for end stage renal disease (ESRD):
- infantile: before 2 years of age
- juvenile (a.k.a. nephronophthisis): most common form, age of onset 10
- adolescent (a.k.a. medullary cystic kidney disease): usually develops in patients in their thirties
- There can be a clinical triad comprising of uraemia, anaemia, and salt wasting (hyponatraemia, hypokalaemia).
- Pathology
- It comprises a group of related conditions characterised by multiple cysts typically at the corticomedullary junction and medulla. The medullary cysts are small. There can be associated atrophy and fibrosis of the basement membrane of the proximal and distal tubules which leads into interstitial fibrosis and end stage renal disease.
- Variants
- familial nephronophthisis:
- autosomal recessive (40%)
- sporadic: non-familial (20%)
- retinal renal syndrome:
- autosomal recessive (15%) associated with retinitis pigmentosa
- adult onset medullary cystic disease:
- autosomal dominant (15%)
- familial nephronophthisis:
- Radiographic features
- Normal to small kidneys with multiple small (<1.5 cm) medullary cysts (sometimes cysts are too small to visualise) at the corticomedullary junction.
What is RF Ablation
Re RCC?
What are the 5 indications?
Radiofrequency Ablation of RCC
- Radiofrequency, cryoablation, and microwave ablation are noninvasive options for treating RCC.
- High-frequency alternating current is applied to a metallic applicator placed within the tumor.
- The surface area of the electrode is small, which results in a high current density at the electrode surface resulting in heat.
- When tissues reach temperatures greater than 50°C, they undergo necrosis.
Indications
- Comorbidities and contraindications to conventional or laparoscopic surgery
- Refusal of conventional surgery
- Compromised renal function
- Patients who have undergone a nephrectomy
- High risk of recurrence (e.g., VHL disease)
What are the imaging features of AML?

Imaging Features
- Fat appears hypodense (CT), hyperechoic (US), and hyperintense (T1W).
- The presence of fat in a renal lesion is virtually diagnostic of AML. There have been only a few case reports of fat in RCC or in oncocytomas.
- Five percent do not demonstrate fat on CT.
- Caveat: be certain that fat associated with a large mass is not trapped in renal sinus or peripheral fat.
- Predominance of blood vessels
- Strong contrast enhancement
- T2W hyperintensity
- Predominance of muscle:
- signal intensity (SI) similar to that of RCC
- AMLs do not contain calcifications;
- if a lesion does contain calcification, consider other diagnosis, such as RCC.
- Angiography:
- tortuous, irregular, aneurysmally dilated vessels are seen in 3%.
- Presence depends on the amount of angiomatous tissue.
- Predominantly myxomatous AMLs may be hypovascular.
Case Discussion
- Predominantly echogenic lesion involving the upper pole of the right kidney associated with more complex appearing perinephric collection.
- CT scan of the abdomen confirms the presence of a fatty lesion in the upper pole of the right kidney consistent with angiomyolipoma complicated by haemorrhage.
- Incidental two tiny hepatic haemangiomas.
- Perirenal haemorrhage without a history of trauma complicating an angiomyolipoma is known as Wunderlich syndrome.
- If perirenal haemorrhage is encountered on ultrasound, a thorough workup should be performed to exclude a bleeding renal cell carcinoma.
- Case courtesy of Dr Hani Makky Al Salam, Radiopaedia.org, rID: 10090
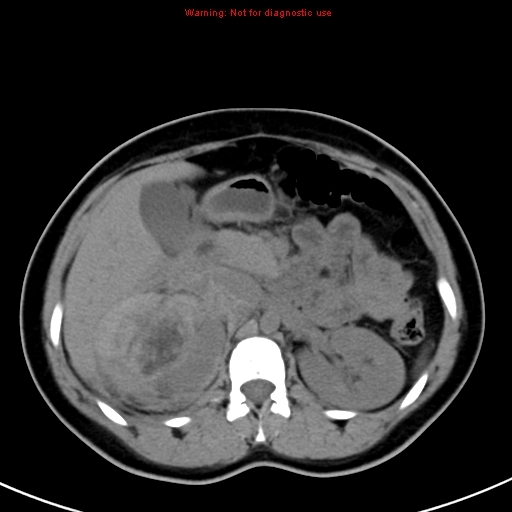
what is this condition
who does it happen to?
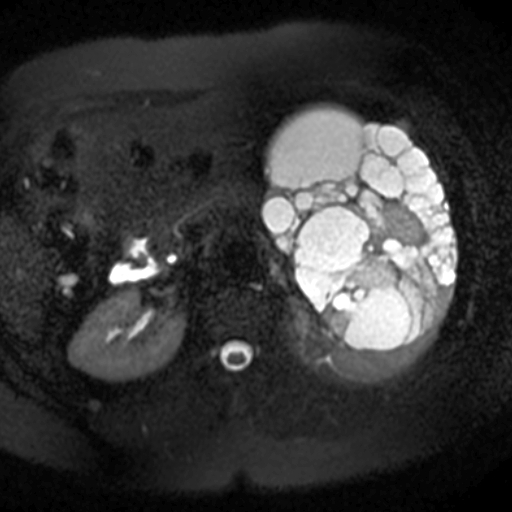
- Cystic nephromas, previously known as multilocular cystic nephromas, are rare benign renal neoplasms classically occurring in adult females in the 4th and 5th decades.
- As of the 2016 WHO classification, they are considered distinct from paediatric cystic nephromas which have associated DICER1 gene mutation 10,11,14.
- All different disorders:
- cystic nephroma (adult)
- paediatric cystic nephroma (paediatric)
- cystic partially differentiated nephroblastoma (paediatric)
- As of 2016, the WHO classifies cystic nephroma within the mixed epithelial and stromal tumour (MEST) family along a spectrum of disease 10,13,14. The remainder of this article will discuss the adult form of cystic nephroma.
- Epidemiology
- overall rare
- adult (typically in the 5th - 6th decades)
- females are predominantly affected
Case courtesy of Dr Roberto Schubert, Radiopaedia.org, rID: 17489
What are are the risk factors for RCC?
What is a/w bilateral tumours?
Risk Factors
- Tobacco use
- Long-term phenacetin use
- VHL disease (bilateral tumors)
- Chronic dialysis (>3 years)
- Family history


























































-
CHEST IMAGING 1100
-
CHEST IMAGING 2100
-
CHEST IMAGING 343
-
CHEST IMAGING 4 (TUMOURS)81
-
CHEST IMAGING 5 PATHOLOGY2
-
CARDIAC IMAGING 1100
-
CARDIAC IMAGING 2100
-
CARDIAC IMAGING 3100
-
CARDIAC IMAGING 443
-
GIT 1101
-
GIT 2100
-
GIT 3100
-
GIT 4102
-
Hepatobilary155
-
Biliary System76
-
Pancreas66
-
Spleen24
-
Adrenal Glands70
-
GENITOURINARY IMAGING 197
-
GENITOURINARY IMAGING 2100
-
GENITOURINARY IMAGING 3100
-
GENITOURINARY IMAGING 4100
-
GENITOURINARY IMAGING 545
-
RETROPERITONEUM33
-
Male Pelvis10
-
GIT PATHOLOGY31
-
Skeletal Dysplasias18
-
MSK104
-
MSK Crack the Core70
-
MSK 295
-
MSK 3100
-
Neuro100
-
Neuro 222
-
NEURO 375
-
Head and Neck 1100
-
Head and Neck 2100
-
Head and Neck 3100
-
Head and Neck 4100
-
Head and Neck 555
-
DDX Head and Neck35
-
Vascular10
-
IR30
-
BREAST IMAGING52
-
OBSTETRICS17
-
GYNAECOLOGY40
-
PAEDIATRICS 196
-
PAEDIATRICS 297
-
PAEDIATRICS 395
-
Nuclear Medicine 134
-
PET CT16
-
Syndromes94
-
HAEMATOLOGY6
-
PATHOLOGY 141
-
Crack the core WHen I Say you say...489
-
Physics31
-
crack the core exam case companion18
-
EPONYMOUS Diseases/signs22
-
What the F&^# is that word?10
-
Radiology Signs25
-
Mnemonics36
-
GIT Pathology1
-
NEURO MRI PHYSICS14
-
GREAT CHEST XRAY CASES1
-
THIS PATIENT IS TYPICAL OF X CONDITION2
