PU/PD has endocrine and non endocrine causes. Outline these:
Endocrine disease
- Diabetes mellitus
- Diabetes insipidus (nephrogenic/central)
- Hyperadrenocorticism
- Hypoadrenocorticism
- Hyperparathyroidism
- Hyperthyroidism
Non-endocrine disease
Renal disease
- AKI/CKD
- Pyelonephritis (upper UTI)
GI disease
- Particularly liver disease – congenital/inflammatory/failure
Genitourinary system
- Infectious/inflammatory disease – pyometra/prostatic abscess
Neurological system
- Inflammatory, traumatic, neoplastic, congenital, psychogenic
Lymphoreticular
- Hyperviscosity – proteins/cells
Pathophysiological processes
- Hypercalcaemia (Neoplasia primarily, inflammatory disease)
- Systemic inflammatory disease (inflammatory leucogram, high level proteins)
- Iatrogenic - medications
From this history and physical exam what do you conclude?
History — Sam is an 11-year-old, 30kg, Labrador with a history of PU/PD for some years. He first became PU/PD around 3 years ago. — The clinical signs persisted for a further 8 months. — A further 3 months elapsed before Sam developed bald patches over his flanks and dorsum. These were non-pruritic and the hair was easily epilated. — A further 9 months elapsed and the owner brought Sam for vaccination having reported that the PU/PD had improved slightly. Unfortunately he had developed moderate left forelimb lameness.
Physical examination:
— Sam was quiet but alert, in lean body condition.
— Vital parameters were within normal limits.
— Oral mucus membranes were pink and moist with a normal CRT.
— Peripheral lymph nodes were within normal limits.
— Ocular mucus membranes were injected, as were the third eyelids.
— Thoracic auscultation was unremarkable.
— Cardiac auscultation was also unremarkable. — Abdominal palpation revealed thin skin but reasonable abdominal contour.
— There were no palpable abdominal abnormalities.
— Dermatological examination revealed a poor haircoat with patchy alopecia, although this was not symmetrical.
Slow onset and long standing condition. Therefore can rule out acute problems like infections and neoplasia as would be dead by 3 years.
Its is waxing and waning so cant be renal as that just gets worse over time. Endocrinopathies can wax and wane. Classic endocrine skin disease because it is non=pruritic because of the high steroids.
Not likely to be thyroid disease because has been going on for a while and most importantly it has PU/PD.
Injected mucous membranes (due to hypertension) and thin skin.
Strong suspicions for endocrinopathy specifically cushings.
So how do we define polydipsia?
Normal water intake:
40-60ml/kg/day
Definition of polydipsia:
>100ml/kg/day
The primary pathophysiologic mechanisms of PU include?
- Defect in osmoregulated ADH secretion (central/cranial/hypothalamic Diabetes insipidus)
- Reduction in the renal response to appropriate circulating concentrations of ADH (nephrogenic Diabetes insipidus)
- Excessive persistent fluid intake (Dipsogenic diabetes insipidus/primary polydipsia/psychogenic polydipsia)
- Osmotic diuresis due to tubular constituents (e.g glucose)
The mechanisms which underpin PUPD?
Primary
- neurogenic/central DI
- nephrogenic DI (rare and presents at birth)
- Dipsogenic DI
Secondary NDI (commonest)
- Interference of action of ADH
- Receptors, generation of cAMP in CD cells
- Renal tubular cell dysfunction, loss of medullary concentrating gradient because medulla gets fibrotic
- Interference with ADH secretion (steroids and phenobarbitone affect this)
How does CKD cause PU/PD?
- Progressive loss of nephrons leads to compensatory changes which lead to further progressive damage.
- Increased fluid load presented to the distal tubules leads to less reabsorption of solutes e.g. urea and electrolytes which results in an osmotic diuresis. In addition changes within the medulla preclude generation of an effective hypertonic interstitium
- In addition tubular changes reduce sensitivity to ADH
How does Hyperadrenocorticism cause PU/PD?
- A variety of mechanisms are suspected to be involved.
- GCs directly interfere with the secretion of ADH at the level of both hypothalamus and pituitary. This is via an increase in osmotic threshold and reduced response of ADH to increasing osmolality.
- GCs are also thought to interfere with ADH action within the distal tubules and collecting ducts. It is also possible that GCs are able to reduce the permeability of the tubules to water.
- In a small number of cases direct compression of the hypothalamus by a pituitary macroadenoma may alter ADH release
How does hypoadrenocorticism cause PU/PD?
- Kidney function is normal in these cases and hypovolaemia may be severe.
- Suspected to be chronic Na wasting and reduction in the concentration gradient within the renal medulla. The influence of hypercalcaemia is also a factor. Ionised hypercalcaemia will lead to a secondary NDI.
- Generally the PD/PU is an early feature of the disease and by the time animals present they are collapsed and have more notable clinical signs associated with GI tract.
- Animals dehydrate due to the sodium wasting from inadequate mineralocorticoid concentrations. This leads to the development of a pre-renal azotaemia despite normal renal function.
How does hypokalaemia cause PU/PD?
- Potassium concentration alters renal blood flow
- This may impair renal tubular potassium-linked transporters preventing solute accumulation in the interstitium and medulla
- There is also a blunting effect of ADH release and rendering of the distal tubule less sensitive to ADH (poss by effect on cAMP generation and downregulation of AQP)
How does hyperthyroidism cause PU/PD?
- Thyroid hormone alters renal blood flow.
- The pathophysiology of PU/PD in hyperthyroidism remains to be ascertained. It is thought possibly to result from increased total medullary blood flow and thus reduced medullary solute concentration
- May also be psychogenic component and many animals suffer concurrent CKD
How does post-obstructive diuresis cause PU/PD?
- Mainly seen in male cats after relief of urethral obstruction
- Marked elevation in urea leads to an osmotic diuresis. This is short lived and self limiting.
How does Glycosuria cause PU/PD?
- Osmotic diuresis due to tubular glucose
- Importantly not all glycosuric animals are diabetic. Recent studies in cats have shown that <30% of cats presented with significant glycosuria to a teaching hospital had causes other than DM.
- Metabolic abnormalities can lead to intermittent/transient glycosuria in some animals. Reports of a number of dogs with fructose intolerance where glycosuria is noted following ingestion of fruit sugars which then resolves when this is cleared.
How does liver disease cause PU/PD?
- Complex relationship with multiple factors responsible
- Impaired urea production reduces medullary tonicity, may also increase GFR.
- Impaired metabolism of ACTH and cortisol
- Impaired metabolism of Aldosterone and NH3
- leads to sodium retention and primary PD
- Psychogenic component may also be present
How does hypercalcaemia cause PU/PD?
- Calcium is thought to exert its influence on the distal tubule via its interaction with ADH via:
- inhibition of adenylate cyclise,
- damage renal tubules directly,
- inhibit binding of ADH to tubules,
- reduce Na/Cl transport in the interstitium
How does pyometra/infection cause PU/PD?
Endotoxins (esp Coli) compete with ADH for binding sites (reversible)
How does Pyelonephritis cause PU/PD?
- Endotoxins (esp Coli) compete with ADH for binding sites
- As above except additional tubular damage may be irreversible
- Inflammation may destroy countercurrent mechanism medulla
How does polycythaemia cause PU/PD?
- Suspected to be due to increased threshold for ADH release which delays response to increasing osmolality
- Thought to be due to increases ANP and baroreceptor stimulation. These inhibit ADH release and CD response to ADH
Where do you start with a PU/PD case?
- In the majority of clinical cases, PD is a result of PU
- A variety of medical conditions induce PD/PU which are COMMON causes
- Primary CDI/NDI are RARE causes
- Primary PD disorders are RARE causes
A minimum database is required to be able to rule in or out common causes of PU/PD. What is this?
- Urinalysis (YOU CAN’T EVALUATE PD/PU WITHOUT IT)
- USG MUST BE MEASURED
- Full analysis including sediment, UPC and culture
- It is important to establish how significant the protein concentration is in the urine
- cystocentesis sample is important after having established the presence of PD/PU
- Serum biochemistry
- Should include urea, creatinine, phosphate, calcium, total protein, glucose, cholesterol, liver enzymes and electrolytes
- Thyroid hormone should be measured in older cats
- CBC to include differential count (not %)
Interpret these results?
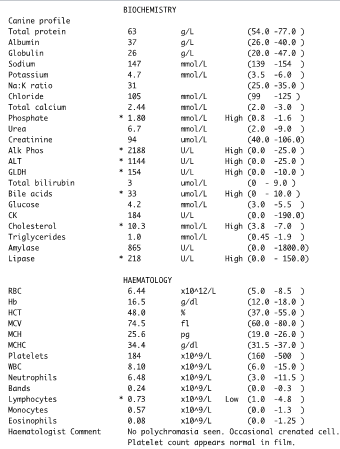
On DDx was liver disease and liver values are up here however in HyperAC you get a metbaollic hepatopathy. Glucocorticoid induced ALP enzyme. This is not an uncommon picture for a cushinoid dog.
Cholesterol increased in dogs with cushings and liver disease would not show high cholesterol.
Classic cushings biochem picture.
Interpret these results?

Metabollic hepatopathy picture seen from endocrinopathies.
Entire female with high levels of progesterone causing type 2 diabetes. She was speyed and weaned off insulin over 3 months and cured.
-
CRS 1 Revision13
-
Infectious Respiratory Disease in Small Animals74
-
Bonzo has a cough..17
-
Freddie has Nasal Discharge26
-
A difficult pet show9
-
ECG revision26
-
Tracheostomy10
-
Coughing in SAs39
-
Foxy Eosinophilic bronchpneumopathy16
-
Help my dog can't breath32
-
Radiology quiz16
-
Thoracic Imaging 263
-
Thoracic imaging 338
-
Respiratory Tract Neoplasia in SA50
-
SA Airway Disease45
-
Approach to LRT Disease in SA48
-
Diseases and Conditions of the Avian Respiratory System47
-
Thoracic Radiography Quiz8
-
Lung Disease Gross Pathology25
-
SA surgery and nasal disease Wrap Up30
-
Respiratory Tract Disease in Small Animals28
-
Pleural Disease54
-
Respiratory Endoscopy35
-
Lower Airway Disease in Cats42
-
Feline Asthma (SDL)15
-
Chest Drains20
-
Sam The Dog Can't Breath6
-
Lung histopathology18
-
Small Animal respiratory parasites39
-
Blood Pressure SDL8
-
Dysrhythmias SDL41
-
SA Endocardial Disease58
-
The Ascitic Dog Cases11
-
Dysrhythmias Management25
-
Feline Cardiomyopathies52
-
Hypertension57
-
Canine Myocardial Disease53
-
Collapse, Weakness, Exercise Intolerance31
-
Cardiac Radiography50
-
Congenital Cardiac Disease48
-
Cyanosis35
-
Radiography of CRS8
-
Management of Heart Failure78
-
Heart Failure Problems10
-
Management Of Heart Failure 223
-
Echocardiograpy Images10
-
Pericardial disease in SA37
-
How to echo33
-
Pericardiocentesis5
-
Thoracic Surgery14
-
Cardiac Cases6
-
Felix11
-
AB selection for respiratory disease37
-
ECG generation14
-
ECG interpretation27
-
CPCR32
-
Triage58
-
Emergency and Critical Cases12
-
Important factors to consider in the emergency and critical care patient27
-
Traumatic Brain Injury38
-
Important factors to consider in the emergency and critical care patient COPY27
-
Nutrition for critically ill patients54
-
Anaesthesia For The Critical Patient: Is It Different?31
-
Critical patients monitoring37
-
CRS ECC Cases20
-
Formative questions46
-
Adrenal glands6
-
Pancreas4
-
Pituitary gland11
-
Thyroid and parathyroid7
-
Hyperglycaemia7
-
Canine hypoadrenocorticism30
-
Canine hyperadrenocorticism37
-
Hepatic lipidosis/ketosis/farm16
-
Feline DM34
-
Canine diabetes mellitus45
-
Diabetic Ketoacidosis27
-
Hypoglycaemia23
-
Feline hyperthyroidism37
-
Canine hypothyroidism34
-
Calcium disorders in SA25
-
Dermatology64
-
Endocrine cases29
-
PU/PD21
-
Uncommon endocrine disorders15
-
Bacterial skin disease43
-
Fungal skin disease22
-
Viral and protozoal skin disease23
-
Parasitic skin disease49
-
Autoimmune and immune mediated diseases of the skin32
-
Practical information14
-
Pattern analysis21
-
Allergic skin disease: pathophysiology and presentation18
-
Management of allergic skin disease29
-
Clinical signs of and approach to pruritus22
-
Appraoch to cutaneous masses35
-
Feline eosinophillic granuloma complexes11
-
Cytology of cutaneous masses28
-
FNA cytology practice7
-
Non-neoplastic masses21
-
Approach to alopecia27
-
Approach to pustular, papular, scaling and crusting skin disease36
-
Otitis48
-
Otitis available treatments and choice15
-
Otic surgery33
-
Dermatological therapeutic case discussion7
-
Feline specific aspects of dermatology18
-
Dermatology cases18
-
SA Anatomy Refresher17
-
Year 2 Formative (Revision)46
-
Introduction5
-
Clinical Approach To GI Disease in SA34
-
Sickly Dog35
-
Vomiting In Dogs and Cats54
-
Gastric Disease in Dogs and Cats57
-
Diagnostic Imaging of GI15
-
Practical: Dog anatomy32
-
SA GI radiography and Ultrasonography71
-
Management of SA oesophageal and gastric SA disease39
-
Pancreatitis43
-
Intro To Intestinal Disease72
-
SI Disorders in Dogs and Cats61
-
Chronic Diarrhoea in SA50
-
Management Plans for Vomiting SA16
-
Devising a Plan12
-
SA Large Intestinal Disease49
-
Why Is This Patient Vomiting Cases27
-
Approach to abdominal radiography21
-
Abdo surgery: intro and biopsy techniques38
-
Abdominal Palpation9
-
Sedation and GI plans for GI patient15
-
Abdominal radiology cases10
-
Weight loss and ascites58
-
Feline Liver Disease72
-
Liver Disease Introduction71
-
Chronic Liver disease in dogs51
-
SA Acute Liver Disease49
-
What Is Wrong With These Patients?19
-
GDV and Gastropexies54
-
Small Animal Acute Abdomen60
-
Abdominal surgery13
-
Feline infectious peritonitis40
-
Gastrotomy, Enterotomy and Enterectomy38
-
Liver, biliary tract and portosystemic shunts48
-
Surgical Diseases of The Oesophagus25
-
Anal and Rectal Conditions66
-
Hernias & Ruptures47
-
Oral tumours, oral surgery & stick injuries50
-
Rabbit Dental Disease15
-
Common Intoxications58
-
Peridontal Disease10
-
Toxiocology cases32
-
Extraction Technique28
-
Oral surgery: surgical extraction technique34
-
GI Disease in Herbivorous Rodents53
-
Formative27
-
Developmental and Genetic Dental Abnormalities9
-
Supporting the Poison Case34
-
Clinical Case10
-
Feline Oral Disease23
-
Pancreatic disease16
-
Bella and her liver16
-
Oral cavity exam33
-
Oral cavity trauma and infection32
-
Introduction COPY4
-
Erythroid110
-
Leukogram62
-
Leukaemia and Lymphadenopathy28
-
Anaemia54
-
Pathology of Lymphoid System58
-
Haemostatic Disease67
-
Diagnosis and Management of Lymphoid Diseases96
-
Immune Mediated Disease64
-
Viruses and Lymphoid System44
-
Blood Transfusions41
-
Formative assessment87
-
Revision practical16
-
Bone pathology51
-
Bone: Diagnostic Imaging70
-
SA MSK Radiography and Radiology20
-
Spine Head and Neck Imaging37
-
Autoimmunity37
-
Principles of Fracture Management 1125
-
Principles of fracture management 2100
-
Case: Bony swelling in dog16
-
NSAIDs58
-
Examination of the Lame Dog and Cat49
-
SA Joint Dx and OA51
-
Sprains and luxations46
-
Joint Treatment6
-
Decision making in Diagnostic Tests CR11
-
Antibiotics51
-
Bones and Joint Histology (and a few pics)28
-
Synoviocentesis7
-
Joint - Inflammatory Conditions60
-
SA bandaging30
-
Triage COPY19
-
Soft Tissue Trauma65
-
Radiology wrap up25
-
Orthopaedic infections46
-
CSGTR Flat Cat10
-
SA developmental disease66
-
SA Developmental Disease Part 260
-
Small Animal Distal Limb78
-
Surgical Planning2
-
Restricting Exercise8
-
SA Muscle Disease27
-
Muscle Pathology10
-
Post Op Managment60
-
SA Hindlimb51
-
SA Forelimb63
-
SA Trauma55
-
Salvage Procedures48
-
Neurodegenerative Disease33
-
Vascular Disease35
-
Neurology Infectious Diseases84
-
Ophthalmic Exam85
-
Conjunctiva and KCS60
-
Corneal Ulcers58
-
Pain Assessment17
-
Non-Notifiable Viral Disease44
-
Notifiable Neuro Viruses26
-
Neuropharmacology47
-
Eye and Disease30
-
Feline Ophthalmology32
-
Behaviour21
-
Ocular Emergencies40
-
Ocular Pharmacology81
-
Toxicities72
-
Inflammatory Disease59
-
Pain Treatment16
-
Neuropathology36
-
Neurosurgery37
-
Exotics Neurology17
-
Pharmacological Control Of Pregnancy and Parturition25
-
Formative COPY43
-
Principles of Pregnancy Failure14
-
Intro to repro pathology137
-
Principles of Cycle Manipulation32
-
Bitch and queen when to spay and why?25
-
Principles of managing dystocia45
-
Monkey (not even a monkey) at the clinic16
-
Approach to Examining the Female Tract42
-
Male Castration63
-
Principles of Contraception42
-
Principles of Neonate Care and Disorders of the Neonate37
-
Principles of therapeutics and anaesthesia in of the neonate and pregnant animal40
-
Reproductive Anaesthesia44
-
Reproductive anaesthesiaCase based seminar13
-
Approach to Examining the Male Reproductive Tract47
-
Reproductive Exam19
-
Facillitator Cases17
-
Spay practical notes28
-
The optimal mating time in the bitch22
-
Urinary Incontinence30
-
Clinical Research - Cystic Endometria Hyperplasia15
-
Diagnostic Methods in the Bitch and Queen82
-
When Will Sasha Have Her Pups?31
-
Abnormalities of pregnancy, parturition and puppies65
-
Abnormalities and Infertility in Female Small Animals45
-
Dystocia Cases31
-
Manipulation of Reproduction and Contraception45
-
Pregnancy Case studies - bitch13
-
First Opinion Reproduction Cases4
-
Unwanted Mating in the Bitch10
-
Pre-pubertal neutering14
-
Bitch Spay Complications21
-
Ovariectomy/Ovariohysterectomy34
-
Surgery of the Female Reproductive Tract34
-
Abnormalities of the Mammary Gland19
-
Peri-operative management and anaesthesia for pyometra in a dog28
-
Common Diseases and Surgery in the Male Dog and Cat37
-
Reproductive Tract Diagnostic Methods and Prostatic Disease in Males76
-
Imaging SA Repro43
-
Exotic reproduction44
-
Repro formative case 16
-
Repro formative case 24
-
Repro formative MCQ23
-
Evaluation of urinary tract disease54
-
Renal Physiology21
-
CKD & AKI26
-
Fluid Therapy9
-
Infectious Diseases7
-
Drug Choices and Therapeutics21
-
Blood Results28
-
Chronic kidney disease79
-
Acute Kidney Injury65
-
Urinary pathology98
-
Urinary Imaging112
-
Fluid therapy in urinary tract disease56
-
Diagnostic approach to polyuria and polydipsia (PUPD)48
-
Neoplasia of Urinary Tract62
-
Congenital And Neonatal Abnormalities82
-
Urinary tract infections39
-
Urinary Tract Disease in Reptiles and Birds85
-
Q and A with steve and jane3
-
Small Animal Urinary Tract Imaging Cases13
-
Interpreting Urinalysis Results48
-
Haematocrit stuff5
-
Crystal quiz9
-
Pu/Pd toolkit20
-
Lower Urinary Tract Disease60
-
Feline Lower Urinary Tract Disease, Calculi and Blocked Cats48
-
Urinary Tract Surgery11
-
Is It Incontinent?8
-
FLUTD7
-
Calculi in Dogs (and Other Pets)18
-
Hypertension/renal failure CR14
-
Practical urinary pathology14
-
FLUTD CR10
-
Contrast Radiographs16
-
Fluid Therapy In Practice36
-
Urinary Incontinence COPY32
-
Principles of urinary surgery53
-
CR Billy the dalmation18
-
Formative MCQ20
-
Formative clinical reasoning6
