- Crusty Jones is a 6 month old female domestic short haired cat
- She is normally seen at another practice but her owners weren’t very happy with the service there so have bought her to you
- She is bright, happy and healthy with a 1cm umbilical hernia BUT her abdomen began to look swollen about a month ago and has got bigger since then.
- She weighs 3kg
- On palpation you can feel what seems to be a soft tissue mass.
- She has no other abnormalities on clinical examination.
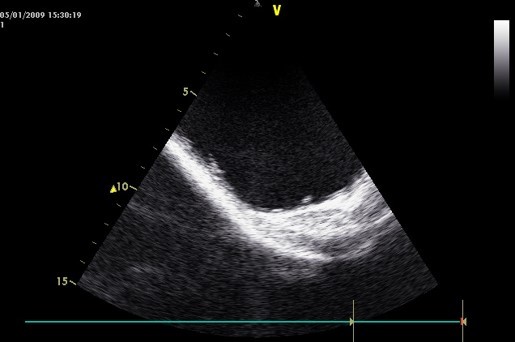
- Using ultrasound you identify a large fluid filled structure cranial to the bladder but cannot characterise it further
- List what would you ideally do next?
–Cystocentesis – ultrasound guided
–Radiography and contrast study?
–Biochem (protein, electrolytes, general health)
- Crusty Jones is a 6 month old female domestic short haired cat
- She is normally seen at another practice but her owners weren’t very happy with the service there so have bought her to you
- She is bright, happy and healthy with a 1cm umbilical hernia BUT her abdomen began to look swollen about a month ago and has got bigger since then.
- She weighs 3kg
- On palpation you can feel what seems to be a soft tissue mass.
- She has no other abnormalities on clinical examination.
- Using ultrasound you identify a large fluid filled structure cranial to the bladder but cannot characterise it further
- After discussion with Mrs Jones and in consideration of the costs of further tests, they ask you perform an exploratory laparotomy without haematology and serum biochemical profile. They want to know if you can spay her at the same time.
- Are you willing to do this? (what are the pros and cons of this)
–Linking 2 major surgeries (more surgery time, higher risk)
–Is on table (already open, saves more incisions)
–Depends on what you find?
- Crusty Jones is a 6 month old female domestic short haired cat
- She is normally seen at another practice but her owners weren’t very happy with the service there so have bought her to you
- She is bright, happy and healthy with a 1cm umbilical hernia BUT her abdomen began to look swollen about a month ago and has got bigger since then.
- She weighs 3kg
Would you like to do a pre-operative biochemistry and haematology screen?
–Ideally especially as pathology not routine, but is young.
- Crusty Jones is a 6 month old female domestic short haired cat
- She is normally seen at another practice but her owners weren’t very happy with the service there so have bought her to you
- She is bright, happy and healthy with a 1cm umbilical hernia BUT her abdomen began to look swollen about a month ago and has got bigger since then.
- She weighs 3kg
- You will also need to choose an anaesthetic protocol for her – calculate the drug dose rates and fluid therapy rates for Crusty
–Pre – med – butorphanorphine (10-20mg/kg) plus ACP? (0.03 - 0.125 mg/kg)
–Leave for 20 mins
–Induction – propofol (6mg/kg)
–Maintenance – isoflurane
Fluids – Hartmann’s at maintenance (2-4ml/kg/hr)
- She is given a buprenorphine premedication 20 minutes before the surgery
- You plan on anaesthetising her with propofol and isoflurane.
- However when the nurse goes to get her out of the cage she doesn’t appear at all sedated and is quite stressed (are you surprised by this)
What else can you/could you give her? Can she have another dose of buprenorphine?
•ACP lower dose (0.03 - 0.125 mg/kg). Would depend on original dose of buprenorphine.
•You ask the nurse to set up an intravenous fluid infusion for the surgery – the nurse is a new trainee and wants to know which fluid and how many seconds per drops per minute she should set the giving set at (your pumps are all occupied with other cases)
Weight 3kg
20 drops/ml
–Take gtt as 20.
–20drops/ml
–4ml/kg/hr x 3 kg = 12ml/hr.
–20drops/ml x 12ml/hr = 240drops/hr
–=4drops/min, or 1 drop every 15 seconds
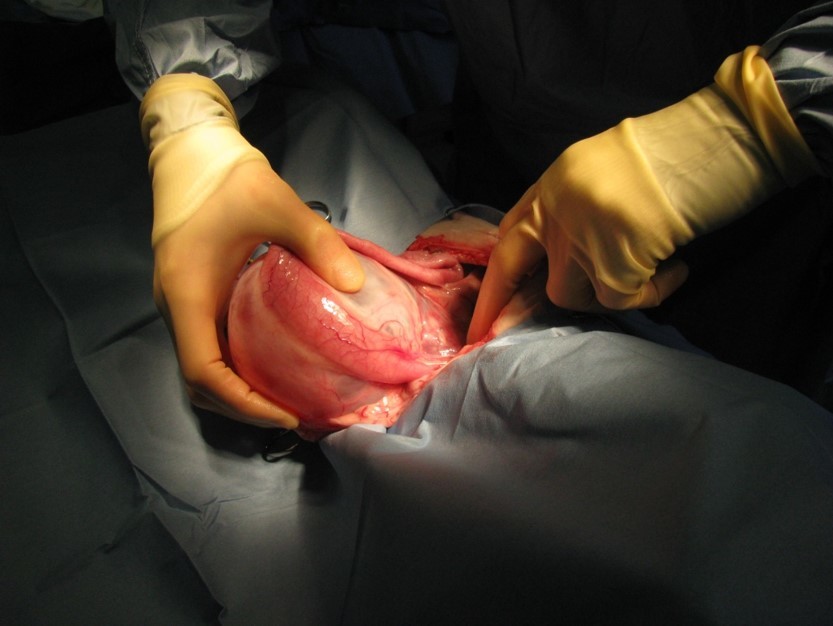
You discover a very enlarged hydronephrotic right kidney her left kidney appears normal
- You have a busy surgery list for the afternoon and the nurse can’t get hold of Mrs Jones on the phone. You are still scrubbed in and the cat is still anaesthetised. You have in-house biochemistry testing available
- You now have to make a decision as to what you should do next make two lists for your notes.
- things you need to consider
- why is it hydronephotic
- blockage?
- Infection
- Congenital
- your options
- Remove the kidney
- Euthanise
- Close and leave
•The kidney has a soft tissue mass;
–How could you biopsy this mass and what are the complications of this?
- Tru-cut.
- Incisional – eliptical, wedge
- Excisional
Complications - bleeding and seeding neoplastic cells
- You contact the owners and get permission for blood tests and nephrectomy. You are feeling very gung-ho today and proceed with the nephrectomy and spay yourself. Owners cannot afford histopathological analysis of kidney.
- She recovers from her anaesthetic normally but is disoriented and seems painful afterwards. She uses her litter tray that evening and produces about 30 ml of urine
- Crusty’s intra-operative blood test results are on the following slides:
- If you had known these results prior to commencing surgery would it have affected your decision to go to surgery or your anaesthetic protocol?
Pct - low
MPV - low
BUN - high
–Small platelets, clotting issues. Mucosal clotting test first?
–Otherwise fine
•What surgical techniques could you have used for the nephrectomy (read the section in Fossum/Tobias on this). Could you do this operation with the standard SVMS surgery kits or would you have needed special equipment?
–Ventral midline abdominal approach, from just behind the xiphoid, extending just caudal to the umbilicus. Retract the intestines, to expose the kidney and its vessels. Incise the peritoneal membrane, to enter the retroperitoneal space. Expose the lateral (convex) surface of the kidney, by blunt and sharp dissection through the retroperitoneal fat. Mobilize the kidney by continued dissection around its cranial, caudal, and dorsal surfaces, until the convex lateral surface can be rotated 90 degrees toward midline. Locate the renal vessels Using hemoclips, or monofilament absorbable suture, double ligate (or clip), and transect, the renal artery Similarly, double ligate and transect the renal vein(s) Incise the retroperitoneum overlying the ureter, and dissect the ureter free over its entire length Routine abdominal closure
•What discharge instructions and long term prognosis will you give her owners after nephrectomy?
–Depends on histo and function of other kidney
-
CRS 1 Revision13
-
Infectious Respiratory Disease in Small Animals74
-
Bonzo has a cough..17
-
Freddie has Nasal Discharge26
-
A difficult pet show9
-
ECG revision26
-
Tracheostomy10
-
Coughing in SAs39
-
Foxy Eosinophilic bronchpneumopathy16
-
Help my dog can't breath32
-
Radiology quiz16
-
Thoracic Imaging 263
-
Thoracic imaging 338
-
Respiratory Tract Neoplasia in SA50
-
SA Airway Disease45
-
Approach to LRT Disease in SA48
-
Diseases and Conditions of the Avian Respiratory System47
-
Thoracic Radiography Quiz8
-
Lung Disease Gross Pathology25
-
SA surgery and nasal disease Wrap Up30
-
Respiratory Tract Disease in Small Animals28
-
Pleural Disease54
-
Respiratory Endoscopy35
-
Lower Airway Disease in Cats42
-
Feline Asthma (SDL)15
-
Chest Drains20
-
Sam The Dog Can't Breath6
-
Lung histopathology18
-
Small Animal respiratory parasites39
-
Blood Pressure SDL8
-
Dysrhythmias SDL41
-
SA Endocardial Disease58
-
The Ascitic Dog Cases11
-
Dysrhythmias Management25
-
Feline Cardiomyopathies52
-
Hypertension57
-
Canine Myocardial Disease53
-
Collapse, Weakness, Exercise Intolerance31
-
Cardiac Radiography50
-
Congenital Cardiac Disease48
-
Cyanosis35
-
Radiography of CRS8
-
Management of Heart Failure78
-
Heart Failure Problems10
-
Management Of Heart Failure 223
-
Echocardiograpy Images10
-
Pericardial disease in SA37
-
How to echo33
-
Pericardiocentesis5
-
Thoracic Surgery14
-
Cardiac Cases6
-
Felix11
-
AB selection for respiratory disease37
-
ECG generation14
-
ECG interpretation27
-
CPCR32
-
Triage58
-
Emergency and Critical Cases12
-
Important factors to consider in the emergency and critical care patient27
-
Traumatic Brain Injury38
-
Important factors to consider in the emergency and critical care patient COPY27
-
Nutrition for critically ill patients54
-
Anaesthesia For The Critical Patient: Is It Different?31
-
Critical patients monitoring37
-
CRS ECC Cases20
-
Formative questions46
-
Adrenal glands6
-
Pancreas4
-
Pituitary gland11
-
Thyroid and parathyroid7
-
Hyperglycaemia7
-
Canine hypoadrenocorticism30
-
Canine hyperadrenocorticism37
-
Hepatic lipidosis/ketosis/farm16
-
Feline DM34
-
Canine diabetes mellitus45
-
Diabetic Ketoacidosis27
-
Hypoglycaemia23
-
Feline hyperthyroidism37
-
Canine hypothyroidism34
-
Calcium disorders in SA25
-
Dermatology64
-
Endocrine cases29
-
PU/PD21
-
Uncommon endocrine disorders15
-
Bacterial skin disease43
-
Fungal skin disease22
-
Viral and protozoal skin disease23
-
Parasitic skin disease49
-
Autoimmune and immune mediated diseases of the skin32
-
Practical information14
-
Pattern analysis21
-
Allergic skin disease: pathophysiology and presentation18
-
Management of allergic skin disease29
-
Clinical signs of and approach to pruritus22
-
Appraoch to cutaneous masses35
-
Feline eosinophillic granuloma complexes11
-
Cytology of cutaneous masses28
-
FNA cytology practice7
-
Non-neoplastic masses21
-
Approach to alopecia27
-
Approach to pustular, papular, scaling and crusting skin disease36
-
Otitis48
-
Otitis available treatments and choice15
-
Otic surgery33
-
Dermatological therapeutic case discussion7
-
Feline specific aspects of dermatology18
-
Dermatology cases18
-
SA Anatomy Refresher17
-
Year 2 Formative (Revision)46
-
Introduction5
-
Clinical Approach To GI Disease in SA34
-
Sickly Dog35
-
Vomiting In Dogs and Cats54
-
Gastric Disease in Dogs and Cats57
-
Diagnostic Imaging of GI15
-
Practical: Dog anatomy32
-
SA GI radiography and Ultrasonography71
-
Management of SA oesophageal and gastric SA disease39
-
Pancreatitis43
-
Intro To Intestinal Disease72
-
SI Disorders in Dogs and Cats61
-
Chronic Diarrhoea in SA50
-
Management Plans for Vomiting SA16
-
Devising a Plan12
-
SA Large Intestinal Disease49
-
Why Is This Patient Vomiting Cases27
-
Approach to abdominal radiography21
-
Abdo surgery: intro and biopsy techniques38
-
Abdominal Palpation9
-
Sedation and GI plans for GI patient15
-
Abdominal radiology cases10
-
Weight loss and ascites58
-
Feline Liver Disease72
-
Liver Disease Introduction71
-
Chronic Liver disease in dogs51
-
SA Acute Liver Disease49
-
What Is Wrong With These Patients?19
-
GDV and Gastropexies54
-
Small Animal Acute Abdomen60
-
Abdominal surgery13
-
Feline infectious peritonitis40
-
Gastrotomy, Enterotomy and Enterectomy38
-
Liver, biliary tract and portosystemic shunts48
-
Surgical Diseases of The Oesophagus25
-
Anal and Rectal Conditions66
-
Hernias & Ruptures47
-
Oral tumours, oral surgery & stick injuries50
-
Rabbit Dental Disease15
-
Common Intoxications58
-
Peridontal Disease10
-
Toxiocology cases32
-
Extraction Technique28
-
Oral surgery: surgical extraction technique34
-
GI Disease in Herbivorous Rodents53
-
Formative27
-
Developmental and Genetic Dental Abnormalities9
-
Supporting the Poison Case34
-
Clinical Case10
-
Feline Oral Disease23
-
Pancreatic disease16
-
Bella and her liver16
-
Oral cavity exam33
-
Oral cavity trauma and infection32
-
Introduction COPY4
-
Erythroid110
-
Leukogram62
-
Leukaemia and Lymphadenopathy28
-
Anaemia54
-
Pathology of Lymphoid System58
-
Haemostatic Disease67
-
Diagnosis and Management of Lymphoid Diseases96
-
Immune Mediated Disease64
-
Viruses and Lymphoid System44
-
Blood Transfusions41
-
Formative assessment87
-
Revision practical16
-
Bone pathology51
-
Bone: Diagnostic Imaging70
-
SA MSK Radiography and Radiology20
-
Spine Head and Neck Imaging37
-
Autoimmunity37
-
Principles of Fracture Management 1125
-
Principles of fracture management 2100
-
Case: Bony swelling in dog16
-
NSAIDs58
-
Examination of the Lame Dog and Cat49
-
SA Joint Dx and OA51
-
Sprains and luxations46
-
Joint Treatment6
-
Decision making in Diagnostic Tests CR11
-
Antibiotics51
-
Bones and Joint Histology (and a few pics)28
-
Synoviocentesis7
-
Joint - Inflammatory Conditions60
-
SA bandaging30
-
Triage COPY19
-
Soft Tissue Trauma65
-
Radiology wrap up25
-
Orthopaedic infections46
-
CSGTR Flat Cat10
-
SA developmental disease66
-
SA Developmental Disease Part 260
-
Small Animal Distal Limb78
-
Surgical Planning2
-
Restricting Exercise8
-
SA Muscle Disease27
-
Muscle Pathology10
-
Post Op Managment60
-
SA Hindlimb51
-
SA Forelimb63
-
SA Trauma55
-
Salvage Procedures48
-
Neurodegenerative Disease33
-
Vascular Disease35
-
Neurology Infectious Diseases84
-
Ophthalmic Exam85
-
Conjunctiva and KCS60
-
Corneal Ulcers58
-
Pain Assessment17
-
Non-Notifiable Viral Disease44
-
Notifiable Neuro Viruses26
-
Neuropharmacology47
-
Eye and Disease30
-
Feline Ophthalmology32
-
Behaviour21
-
Ocular Emergencies40
-
Ocular Pharmacology81
-
Toxicities72
-
Inflammatory Disease59
-
Pain Treatment16
-
Neuropathology36
-
Neurosurgery37
-
Exotics Neurology17
-
Pharmacological Control Of Pregnancy and Parturition25
-
Formative COPY43
-
Principles of Pregnancy Failure14
-
Intro to repro pathology137
-
Principles of Cycle Manipulation32
-
Bitch and queen when to spay and why?25
-
Principles of managing dystocia45
-
Monkey (not even a monkey) at the clinic16
-
Approach to Examining the Female Tract42
-
Male Castration63
-
Principles of Contraception42
-
Principles of Neonate Care and Disorders of the Neonate37
-
Principles of therapeutics and anaesthesia in of the neonate and pregnant animal40
-
Reproductive Anaesthesia44
-
Reproductive anaesthesiaCase based seminar13
-
Approach to Examining the Male Reproductive Tract47
-
Reproductive Exam19
-
Facillitator Cases17
-
Spay practical notes28
-
The optimal mating time in the bitch22
-
Urinary Incontinence30
-
Clinical Research - Cystic Endometria Hyperplasia15
-
Diagnostic Methods in the Bitch and Queen82
-
When Will Sasha Have Her Pups?31
-
Abnormalities of pregnancy, parturition and puppies65
-
Abnormalities and Infertility in Female Small Animals45
-
Dystocia Cases31
-
Manipulation of Reproduction and Contraception45
-
Pregnancy Case studies - bitch13
-
First Opinion Reproduction Cases4
-
Unwanted Mating in the Bitch10
-
Pre-pubertal neutering14
-
Bitch Spay Complications21
-
Ovariectomy/Ovariohysterectomy34
-
Surgery of the Female Reproductive Tract34
-
Abnormalities of the Mammary Gland19
-
Peri-operative management and anaesthesia for pyometra in a dog28
-
Common Diseases and Surgery in the Male Dog and Cat37
-
Reproductive Tract Diagnostic Methods and Prostatic Disease in Males76
-
Imaging SA Repro43
-
Exotic reproduction44
-
Repro formative case 16
-
Repro formative case 24
-
Repro formative MCQ23
-
Evaluation of urinary tract disease54
-
Renal Physiology21
-
CKD & AKI26
-
Fluid Therapy9
-
Infectious Diseases7
-
Drug Choices and Therapeutics21
-
Blood Results28
-
Chronic kidney disease79
-
Acute Kidney Injury65
-
Urinary pathology98
-
Urinary Imaging112
-
Fluid therapy in urinary tract disease56
-
Diagnostic approach to polyuria and polydipsia (PUPD)48
-
Neoplasia of Urinary Tract62
-
Congenital And Neonatal Abnormalities82
-
Urinary tract infections39
-
Urinary Tract Disease in Reptiles and Birds85
-
Q and A with steve and jane3
-
Small Animal Urinary Tract Imaging Cases13
-
Interpreting Urinalysis Results48
-
Haematocrit stuff5
-
Crystal quiz9
-
Pu/Pd toolkit20
-
Lower Urinary Tract Disease60
-
Feline Lower Urinary Tract Disease, Calculi and Blocked Cats48
-
Urinary Tract Surgery11
-
Is It Incontinent?8
-
FLUTD7
-
Calculi in Dogs (and Other Pets)18
-
Hypertension/renal failure CR14
-
Practical urinary pathology14
-
FLUTD CR10
-
Contrast Radiographs16
-
Fluid Therapy In Practice36
-
Urinary Incontinence COPY32
-
Principles of urinary surgery53
-
CR Billy the dalmation18
-
Formative MCQ20
-
Formative clinical reasoning6
